Walk into any supplement shop and vitamin D sits on the shelf next to creatine, sold with the same tone. Better strength. Better recovery. Better immunity. Better testosterone. Better everything.
The actual research is much narrower.
Vitamin D matters. It is genuinely essential. It plays a role in calcium absorption, bone remodeling, immune function, and (yes) muscle. When people are deficient, supplementing fixes real problems. But the question most readers are actually asking is different. If I take a vitamin D pill, will it make me stronger, faster, or healthier than I already am? Across the strongest available evidence, the answer is mostly no, with one specific exception.
This article walks through what the 2024 athlete meta-analysis actually found, why insufficiency is more common than people think, why the falls-and-fractures story collapsed in 2018, and what the new Endocrine Society guideline tells healthy adults to do.
The Athlete Trial: Han et al. (2024)
The most rigorous recent evidence on vitamin D and athletic strength is the systematic review and meta-analysis by Han, Xiang, An, Tan, Shao, and Wang (2024) in Frontiers in Nutrition. The authors searched the major databases, screened the available randomized controlled trials, and pooled 10 RCTs with 318 athletes who completed the study protocols (166 in the vitamin D3 group, 152 in placebo).
The dosing across these trials varied widely. Daily protocols ranged from 2,000 IU all the way up to roughly 18,750 IU per day for 4 to 12 weeks, with most studies clustering at the lower end of that range. One trial used a single 150,000 IU bolus. Across the pool, vitamin D3 supplementation reliably raised serum 25(OH)D by an average of 14.76 ng/mL (p<0.0001). The pills worked. The question was whether the raised vitamin D status actually carried over to performance.
What They Found for Lower-Limb Strength
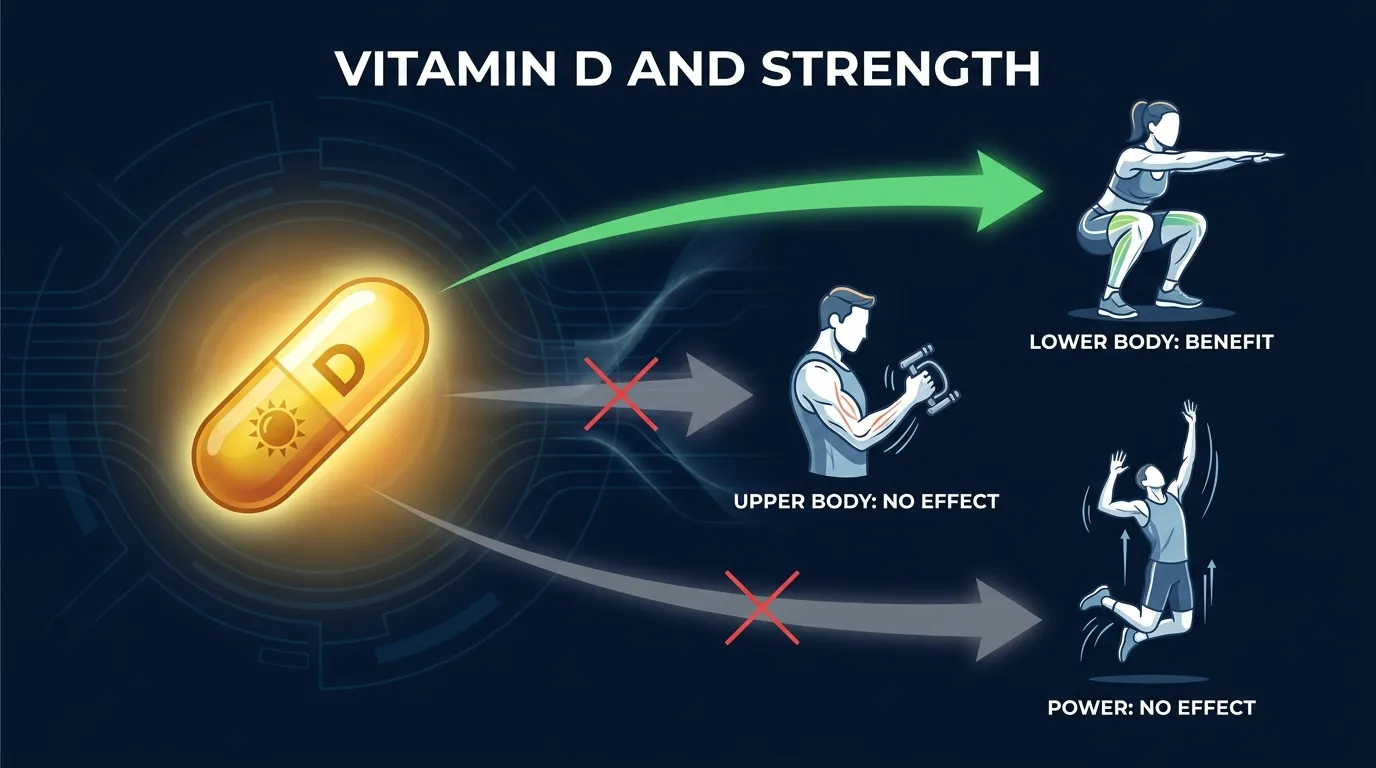
This is the one positive result. Pooling the trials that measured quadriceps contraction strength, vitamin D3 produced a standardized mean difference of 0.57 (95 percent CI 0.04 to 1.11, p=0.04). That is a small-to-moderate effect. Not nothing. Worth taking seriously for someone whose squat strength matters and whose status is low.
What They Found for Everything Else
The other strength and power outcomes did not budge:
- Handgrip (upper-limb strength): SMD 0.21 (95 percent CI -0.23 to 0.64, p=0.35). No effect.
- Vertical jump (explosive power): SMD 0.21 (95 percent CI -0.09 to 0.50, p=0.17). No effect.
- Bench press 1-rep max: SMD -0.15 (95 percent CI -0.57 to 0.26, p=0.47). No effect.
- Overall combined strength: SMD 0.18, p=0.08. Trending positive, not significant.
So the headline is specific. Vitamin D3 supplementation appears to help quadriceps-type lower-body strength in athletes. It does not appear to help the upper body, and it does not appear to help power.
Baseline Status Matters
The other important detail buried in the subgroup analysis: the benefit concentrated in athletes who started insufficient. Athletes whose baseline 25(OH)D was below 30 ng/mL gained more from supplementation. Athletes who were already sufficient saw little to no benefit. This is consistent with how most nutritional micronutrients work. The pill corrects a shortage. It does not create a surplus benefit.
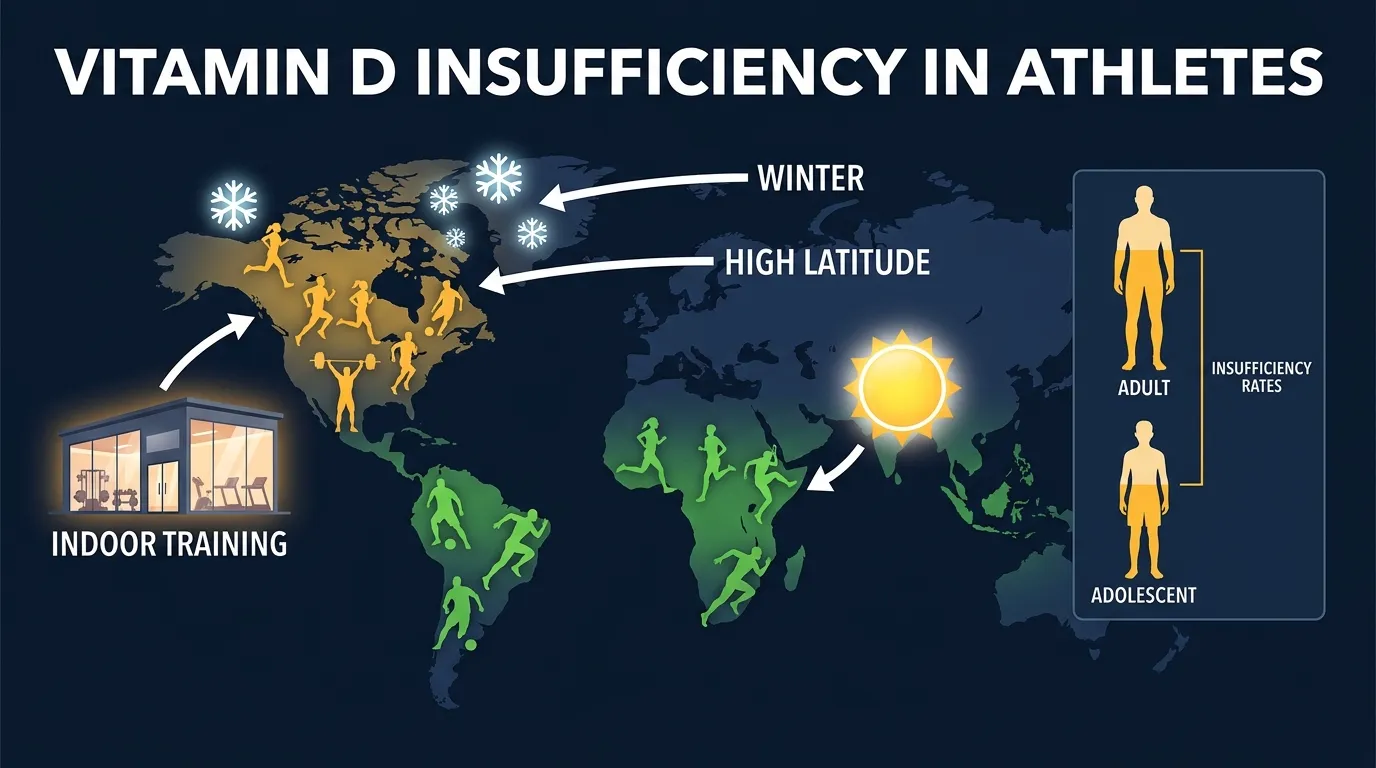
If you train indoors, train in winter at high latitude, or have darker skin, you are more likely to be in that insufficient group. The meta-analysis specifically called out that vitamin D3 was more effective in athletes who trained indoors.
How Common Is Insufficiency in Athletes?
Pretty common. The 2022 systematic review by Harju, Gray, Mavroedi, Farooq, and Reilly in the European Journal of Nutrition pooled 51 prevalence studies and 5,456 elite athletes from around the world. Their headline numbers:
- About 30 percent of adult elite athletes had insufficient vitamin D (serum 25(OH)D below 50 nmol/L).
- About 39 percent of adolescent elite athletes were insufficient.
- Insufficiency was higher in winter, at higher latitudes, and in indoor sports.
- Sex did not significantly change the risk (RR 1.0, 95 percent CI 0.79 to 1.26).
Two takeaways from that. First, if you are an athlete and you have never had your 25(OH)D checked, there is roughly a 1-in-3 chance you are insufficient. Second, even if you train hard outdoors in summer, the pattern is seasonal. Winter pulls almost everyone in northern climates below the threshold by February.
One caveat. Harju et al. studied elite athletes, not recreational gym-goers. The prevalence in the general adult population is similar in size, per NIH data, but the populations are not identical.
Get an evidence-based plan built for you
FitCraft, our mobile fitness app, pairs you with an AI coach who builds you a personalized plan around your goals, schedule, and fitness level. Every FitCraft program is designed by Domenic Angelino, MPH (Brown University) and NSCA-CSCS, with research published in the Journal of Strength and Conditioning Research and Medicine & Science in Sports & Exercise.
Take the Free Assessment Free • 2 minutes • No credit cardThe Falls-and-Fractures Story Collapsed in 2018
For about two decades, vitamin D was sold to older adults as a fall-prevention and fracture-prevention supplement. The story was intuitive. Older people are often low in D. Low D might weaken muscle and bone. Pills should help.
Then the bigger trials came in.
The 2018 meta-analysis by Bolland, Grey, and Avenell in The Lancet Diabetes & Endocrinology pooled 81 randomized controlled trials of vitamin D supplementation, totaling 53,537 participants. The results were striking in their flatness:
- Total fractures: relative risk 1.00 (95 percent CI 0.93 to 1.07). No effect.
- Hip fractures: relative risk 1.11 (95 percent CI 0.97 to 1.26). Possibly even slightly worse.
- Falls: relative risk 0.97 (95 percent CI 0.93 to 1.02). No effect.
- Bone mineral density: -0.16 percent to +0.76 percent across 1 to 5 years. Not clinically meaningful.
And higher doses did not work better than lower doses. The authors concluded that "vitamin D supplementation does not prevent fractures or falls, or have clinically meaningful effects on bone mineral density." This conclusion is contested at the edges (some researchers argue calcium-plus-D combinations were unfairly excluded), but the core finding has held up. The big subsequent trials (VITAL, D2d, ViDA) also failed to show meaningful benefit in generally well-nourished populations.
This is also where the modern guideline picture comes from.
What the 2024 Endocrine Society Guideline Says
The most recent authoritative recommendation is the 2024 clinical practice guideline by Demay, Pittas, Bikle, and colleagues in the Journal of Clinical Endocrinology & Metabolism. The expert panel reviewed the available evidence and issued recommendations for distinct populations:
- Healthy adults 19 to 74: the panel suggests against routine vitamin D supplementation beyond the RDA, and against routine 25(OH)D blood testing. The trials simply have not shown disease-prevention benefits in this group.
- Adults 75 and older: the panel suggests empiric daily vitamin D supplementation. The reasoning is a mortality signal in trials, not a falls or fractures benefit.
- Children and pregnant individuals: empiric supplementation suggested, mostly for rickets prevention and pregnancy-specific outcomes.
- Adults with prediabetes: empiric vitamin D suggested, based on diabetes-progression trials.
The RDA the guideline points to is the Institute of Medicine standard: 600 IU per day for adults 19 to 70, and 800 IU per day for adults 71 and older. The tolerable upper intake level for healthy adults is 4,000 IU per day, per the NIH Office of Dietary Supplements.
This is a meaningful shift. The guideline before this (from 2011) recommended much higher targets and broader screening. The new one pulls back. The underlying reason is the same as the falls-and-fractures story. The big trials did not show what people hoped they would show.
Where Vitamin D Probably Still Matters
Saying the supplement story has been overhyped is not the same as saying the nutrient does not matter. There are populations and situations where vitamin D is genuinely worth thinking about.
True Deficiency
People with serum 25(OH)D below 20 ng/mL (50 nmol/L) are deficient, and below 12 ng/mL (30 nmol/L) is severe. At those levels you get real problems: bone pain, muscle weakness, increased infection susceptibility, and over years, osteomalacia in adults or rickets in children. Correcting deficiency with supplementation is well-supported and not really controversial. The Endocrine Society guideline is about healthy adults, not deficient ones.
People at elevated deficiency risk include: those with darker skin in northern latitudes, indoor workers, people who cover most of their skin for cultural or medical reasons, those with malabsorption conditions (Crohn's, celiac, gastric bypass), those on certain anticonvulsants or glucocorticoids, and adults with obesity. If you fit into one of these categories, ask your doctor about a 25(OH)D check.
Athletes With Insufficiency
Per Han et al. (2024), if you are an athlete and your baseline 25(OH)D is below 30 ng/mL, correcting it with 2,000 to 5,000 IU per day for several weeks can give you a small lower-limb strength bump. That is real, just not huge. It is also a one-time recovery from a deficit, not a permanent boost. Once your serum level normalizes, ongoing supplementation does not keep stacking benefits.
Older Adults
For people 75 and older, the 2024 Endocrine Society guideline does suggest empiric daily vitamin D supplementation. The reasoning is a mortality signal across pooled trials, not a falls or fractures effect. Daily lower-dose formulations are preferred over the older "monthly mega-dose" approach. Some monthly bolus trials actually showed slight harm.
How Much, From Where, and When
If you decide to supplement, the dosing landscape is simple.
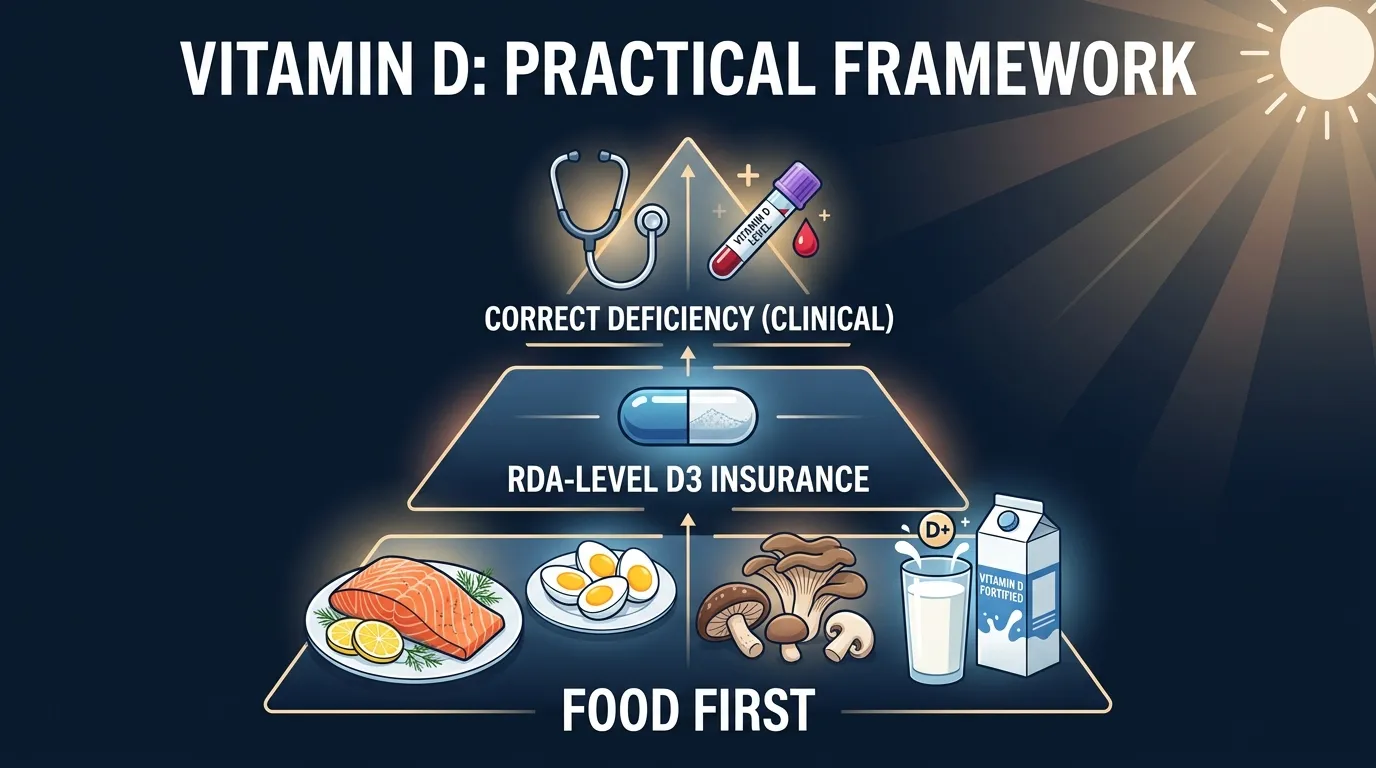
Food First
The natural-food list for vitamin D is short, which is partly why supplementation became so popular. Per the NIH Office of Dietary Supplements, the best sources are:
- Fatty fish (salmon, trout, sardines, mackerel): roughly 400 to 800 IU per 3-ounce serving.
- Cod liver oil: about 1,360 IU per tablespoon.
- UV-exposed mushrooms: 100 to 400 IU per half cup, depending on the variety and how they were treated.
- Egg yolks: about 40 IU per large yolk.
- Fortified dairy and plant milks: about 100 IU per cup in the US.
- Fortified breakfast cereals: 40 to 100 IU per serving.
About 30 minutes of midday sun on uncovered arms and legs in summer can also produce roughly 1,000 IU of skin-synthesized D in lighter-skinned adults. The number is lower in darker skin, at higher latitudes, with sunscreen, and in winter. For most northern-latitude adults from October to March, sun alone is not enough.
If You Supplement
The RDA-aligned approach for healthy adults is straightforward:
- 600 IU per day if you are 19 to 70.
- 800 IU per day if you are 71 or older.
- Up to 4,000 IU per day is the tolerable upper intake level for healthy adults. Stay below it unless your doctor is monitoring.
- Vitamin D3 (cholecalciferol) is the form used in essentially all the athlete strength trials and most musculoskeletal trials. It raises serum 25(OH)D more efficiently than D2.
- Take it with a fatty meal for better absorption. Vitamin D is fat-soluble.
- Daily dosing beats weekly or monthly mega-doses, per the Endocrine Society guideline. Big bolus protocols have failed to show benefit and in some trials caused harm.
If you suspect actual deficiency (you have the risk factors above, or you have symptoms), ask your doctor for a 25(OH)D test. Correcting a documented low level is the one scenario where a higher dose for a defined period is well-supported.
What This Means If You Are Just Trying to Get Stronger
Here is the honest summary for the average reader who lifts a few times a week and is wondering whether to buy a bottle:
If you eat fatty fish twice a week, get some sunlight in summer, and use fortified dairy, you probably do not need a supplement. If you train indoors, live somewhere with real winter, and rarely eat fatty fish, a 1,000 to 2,000 IU per day daily dose is reasonable insurance. It will not give you a meaningful lower-body strength boost unless your starting status is below 30 ng/mL. It will not boost your upper-body strength or your power at all. It will not protect your bones beyond a normal-diet baseline. And taking more is not better.
The bigger lever for strength is the obvious one: progressive resistance training, enough protein, and consistent sleep. Vitamin D is a small support player. The pattern matches what we see for almost every supplement category covered in our other writeups: the magnesium and muscle cramps story, the caffeine and performance picture, even the creatine brain benefits evidence. Real signal exists in narrow places. The supplement-aisle story is usually broader than the evidence supports.
How FitCraft Treats Nutrition and Strength
Most fitness apps either pretend supplements solve everything or ignore nutrition entirely. Neither is honest.
FitCraft pairs you with an AI coach who builds your plan around the goals and constraints you share at signup. The training side is structured progressively, which is where the real lower-body strength gains actually come from. For nutrition questions, the right move is the boring one: get the basics from food, supplement narrowly where the evidence is decent and the cost is low (D in winter for indoor athletes, creatine monohydrate, caffeine before sessions), and skip everything else.
References
- Han Q, Xiang M, An N, Tan Q, Shao J, Wang Q. "Effects of vitamin D3 supplementation on strength of lower and upper extremities in athletes: an updated systematic review and meta-analysis of randomized controlled trials." Frontiers in Nutrition. 2024;11:1381301. doi:10.3389/fnut.2024.1381301
- Harju T, Gray B, Mavroedi A, Farooq A, Reilly JJ. "Prevalence and novel risk factors for vitamin D insufficiency in elite athletes: systematic review and meta-analysis." European Journal of Nutrition. 2022;61(8):3857-3871. doi:10.1007/s00394-022-02967-z
- Bolland MJ, Grey A, Avenell A. "Effects of vitamin D supplementation on musculoskeletal health: a systematic review, meta-analysis, and trial sequential analysis." The Lancet Diabetes & Endocrinology. 2018;6(11):847-858. doi:10.1016/S2213-8587(18)30265-1 (PMID 30293909).
- Demay MB, Pittas AG, Bikle DD, et al. "Vitamin D for the Prevention of Disease: An Endocrine Society Clinical Practice Guideline." Journal of Clinical Endocrinology & Metabolism. 2024;109(8):1907-1947. doi:10.1210/clinem/dgae290
- National Institutes of Health Office of Dietary Supplements. "Vitamin D Fact Sheet for Health Professionals." ods.od.nih.gov/factsheets/VitaminD-HealthProfessional/
Frequently Asked Questions
Does vitamin D actually make you stronger?
Modestly, and only in some muscle groups. A 2024 meta-analysis by Han et al. in Frontiers in Nutrition pooled 10 randomized controlled trials of 318 athletes. Lower-limb strength (quadriceps) improved with vitamin D3 supplementation by a small-to-moderate amount (standardized mean difference 0.57, p=0.04). Upper-limb strength (handgrip), bench press 1-rep max, and explosive power (vertical jump) did not improve at all. The benefit also tracked baseline status: athletes who started below 30 ng/mL (insufficient) got the gains. Athletes who already had sufficient levels saw little to no effect. If your serum 25(OH)D is already normal, taking more vitamin D will not make you stronger.
How common is vitamin D insufficiency in athletes?
More common than most people guess. A 2022 systematic review by Harju et al. in the European Journal of Nutrition pooled 51 studies and 5,456 elite athletes. About 30 percent of adult athletes and 39 percent of adolescent athletes had insufficient vitamin D (serum 25(OH)D below 50 nmol/L). Risk goes up in winter, at higher latitudes, and in athletes who train indoors. Sex did not matter much. So even if you train hard outdoors in summer, you can still be insufficient by February.
How much vitamin D should I take?
For most healthy adults, hit the RDA: 600 IU per day if you are 19 to 70, and 800 IU per day if you are 71 or older. The 2024 Endocrine Society guideline (Demay et al., JCEM) recommends against routine higher-dose supplementation in healthy adults under 75, and also recommends against routine 25(OH)D blood testing in the same group. The trials underlying RCT-level meta-analyses on athletes used daily doses ranging from 2,000 IU to roughly 18,750 IU for 4 to 12 weeks, with most studies clustering at 2,000 to 5,000 IU per day to correct insufficiency. The NIH-set tolerable upper intake level for adults is 4,000 IU per day. Higher doses are sometimes prescribed for documented deficiency, but should be supervised by your doctor.
Does vitamin D prevent falls and fractures in older adults?
On the strongest available evidence, no. A 2018 Lancet Diabetes & Endocrinology meta-analysis by Bolland, Grey, and Avenell pooled 81 randomized trials and 53,537 participants. Vitamin D supplementation showed no effect on total fractures (RR 1.00), hip fractures (RR 1.11), or falls (RR 0.97). Bone mineral density changes were under 1 percent across 1 to 5 years, not clinically meaningful. Higher doses did not work better than lower doses. There is one important exception: people with true deficiency, rickets, or osteomalacia do benefit from supplementation. The 2024 Endocrine Society guideline does make a separate empiric supplementation suggestion for adults 75+ based on a mortality signal, but not because falls or fractures were reduced.
What foods are highest in vitamin D?
Vitamin D is one of the harder nutrients to get from food because the natural food list is short. The NIH Office of Dietary Supplements lists fatty fish (salmon, trout, sardines, mackerel) at 400 to 800 IU per 3-ounce serving, cod liver oil at about 1,360 IU per tablespoon, egg yolks at around 40 IU per large yolk, and UV-exposed mushrooms at 100 to 400 IU per half cup. Most US milk is fortified to about 100 IU per cup, and many breakfast cereals add 40 to 100 IU per serving. If you eat fatty fish twice a week and use fortified dairy, you are probably close to the RDA. If you do not, food alone often will not get you there in winter.