- One workout buys you 24 to 48 hours. A single bout of moderate or vigorous exercise raises whole-body insulin sensitivity for roughly one to two days, then it fades back. Bird and Hawley (BMJ Open SEM, 2017) summarized the literature on the acute-versus-chronic split.
- Training is a real intervention. Way et al. (Diabetes & Metabolism Journal, 2016) pooled randomized trials in type 2 diabetes and found insulin resistance dropped with a pooled effect size of -0.588. That sits in the same range as many first-line medications.
- Resistance training rewires the muscle. Croymans et al. (J Appl Physiol, 2013) found 12 weeks of resistance training raised skeletal muscle GLUT4 protein and improved muscle insulin sensitivity in overweight, sedentary young men.
- Breaking up sitting works on its own. Dunstan et al. (Diabetes Care, 2012) showed that interrupting prolonged sitting every 20 minutes with a 2-minute walk cut postprandial insulin by 23% versus uninterrupted sitting.
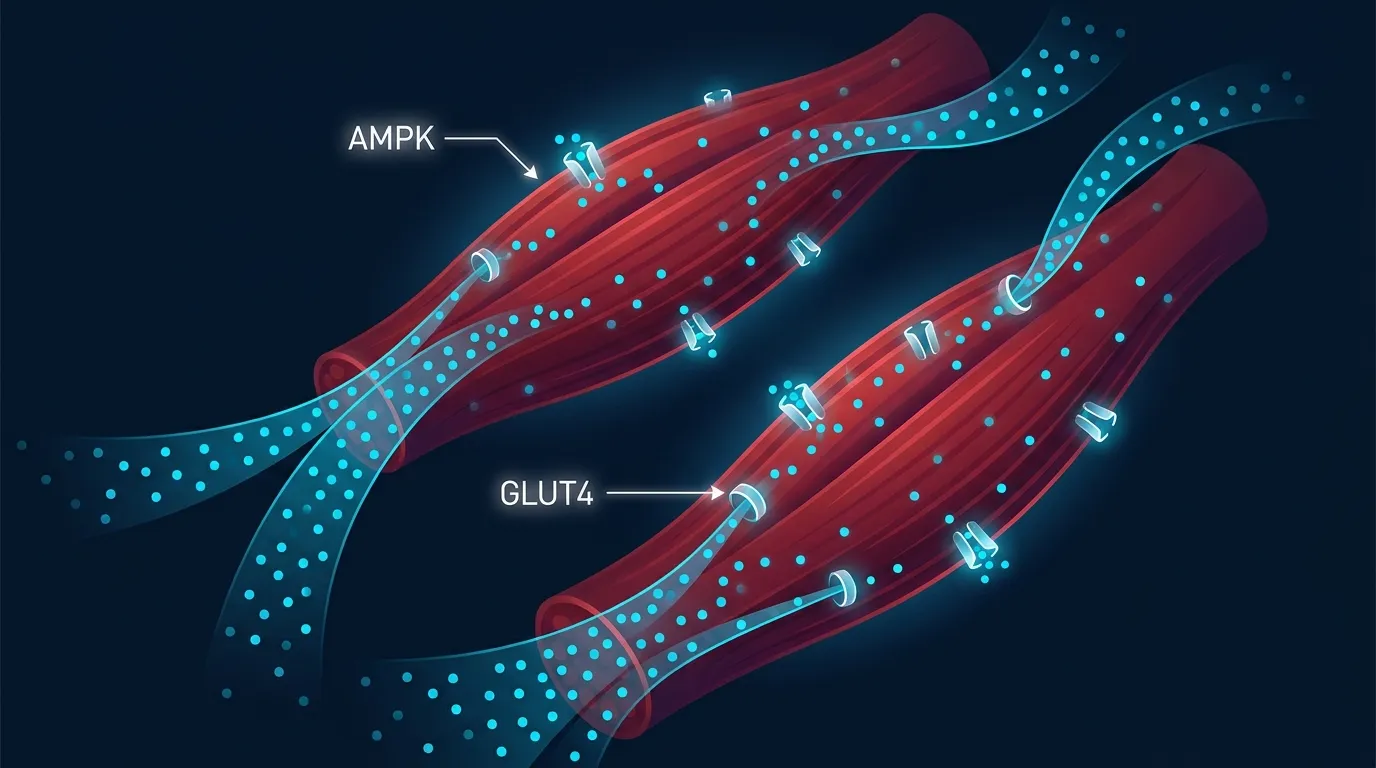
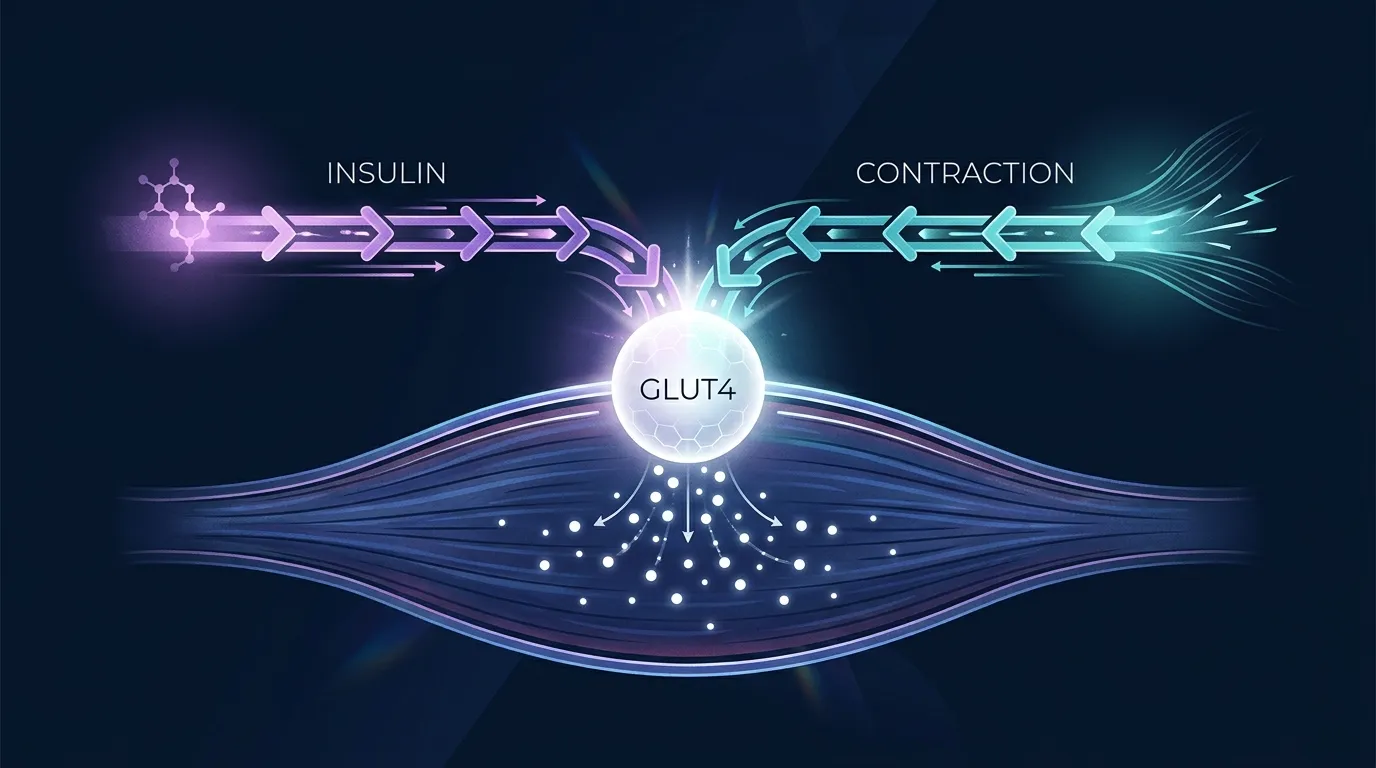
- Mechanism: contraction pulls glucose without insulin. Working muscle translocates GLUT4 to the cell membrane through AMPK, independent of the insulin pathway. That is why exercise works even when insulin signaling is broken.
Insulin sensitivity is one of the cleanest biomarkers in human physiology, and it moves more with exercise than with almost any other lifestyle lever. A single workout makes your muscles meaningfully more responsive to insulin for the next day or two. Train consistently for 12 weeks and the effect becomes structural. The muscle itself changes.
What's striking is how fast it works. You don't need months. You need one decent session and then another one before the first one wears off. That's the entire framework.
The rest of this article walks through what the trials actually found. We'll cover the acute effect of a single bout, the chronic effect of consistent training, how resistance training and aerobic training stack up, and the surprising role of just standing up more often. Then we'll close with the practical dose.
The Research: What Studies Show
Four lines of evidence carry most of the weight here. Acute single-bout studies. Long-term aerobic training trials. Resistance training trials. And the newer interrupting-sitting literature. The pattern across all four is consistent, which is unusual in exercise research.
The Acute Effect: One Bout Lasts 24 to 48 Hours
A useful starting point is the review by Bird and Hawley (2017), published in BMJ Open Sport & Exercise Medicine. The paper synthesizes the literature on how a single exercise session changes insulin sensitivity and how the effect changes with chronic training. The authors document that a single bout of moderate or vigorous exercise transiently raises whole-body insulin sensitivity, with the effect detectable within hours and persisting for roughly 24 to 48 hours before it fades.
The mechanism is two-pronged. During and immediately after exercise, contracting muscle takes up glucose through an insulin-independent pathway (more on this below). Then in the recovery window, the muscle becomes hypersensitive to insulin itself, partly through prolonged phosphorylation of the proteins TBC1D1 and TBC1D4 that sit downstream of insulin signaling. Insulin works better on a muscle that exercised yesterday.
This explains a result that surprises a lot of people. You cannot bank insulin sensitivity. A killer Saturday workout doesn't carry you through Wednesday. By Monday afternoon the acute effect is largely gone. The interventions that move long-term metabolic markers do so by stacking sessions close enough together that the acute effects overlap and become a baseline state.
Way 2016: The Pooled Effect in Type 2 Diabetes
The best single estimate for how big a deal this is in a clinical population comes from Way and colleagues (2016) in the Diabetes & Metabolism Journal. The team ran a systematic review and meta-analysis of randomized controlled trials of regular exercise training in adults with type 2 diabetes. They pooled the studies that measured insulin sensitivity or insulin resistance as an outcome and ran a standardized effect-size analysis.
The pooled effect size for insulin resistance reduction was -0.588 (95% confidence interval -0.816 to -0.359). In plain language, that is a moderate-to-large effect, statistically robust, and broadly comparable to what you see from many first-line glucose-lowering medications. Both aerobic and resistance training delivered the benefit. Longer interventions tended to produce larger effects.
This is the number to remember when someone asks "does it actually matter that much." Yes. In the population where it matters most (adults with established type 2 diabetes), regular training produces a clinically meaningful drop in insulin resistance, on the same order as a medication intervention.
Croymans 2013: Resistance Training Rebuilds the GLUT4 Machinery
Croymans and colleagues (2013), in the Journal of Applied Physiology, took a closer look at what resistance training does to the muscle itself. The team put overweight, sedentary young men through a 12-week, supervised, full-body resistance program. They measured oral indices of muscle insulin sensitivity, beta-cell function, and (via biopsy) skeletal muscle protein content of GLUT4, the transporter that does the actual glucose-uptake work.
By the end of the 12 weeks, oral indices of muscle insulin sensitivity had improved, beta-cell function had improved, and skeletal muscle GLUT4 protein content had gone up. Resistance training, in other words, doesn't just acutely tickle the system. It expands the underlying capacity to dispose of glucose by putting more GLUT4 protein in the muscle.
That structural change is the part that compounds. The acute bout matters for the next 24 to 48 hours. The chronic adaptation matters every day, indefinitely, as long as you keep training. A bigger, more GLUT4-rich muscle is a bigger glucose sink at rest. That is why the same person can eat the same meal at age 30 and at age 45 and get a much higher glucose spike at 45 if they've lost the muscle.
Dunstan 2012: Breaking Up Sitting Counts
The newest piece of the picture is the sitting-interruption literature, anchored by Dunstan and colleagues (2012) in Diabetes Care. The team had 19 overweight and obese adults complete three randomized 5-hour conditions: uninterrupted sitting, sitting interrupted every 20 minutes with a 2-minute bout of light-intensity walking, and sitting interrupted every 20 minutes with a 2-minute bout of moderate-intensity walking. All three conditions included two standardized test meals.
Both walking-break conditions cut postprandial glucose by about 24% and postprandial insulin by 23% versus uninterrupted sitting. The intensity barely mattered. Light and moderate walking produced almost identical effects on glucose and insulin, suggesting it is the act of repeatedly turning the muscle on (not the cardiovascular demand) that does the work.
This finding has gotten progressively more attention because it changes the framing of "how do I exercise enough." A sedentary day with three 2-minute walks per hour is not the same metabolic environment as a sedentary day with no breaks, even if the total movement time is small. The high-leverage intervention may not be the workout you scheduled at 6pm. It may be the dozen short standups during the workday.
Why This Matters for Your Fitness
Insulin sensitivity is doing more work in your body than the name suggests. When it drops, glucose stays elevated longer after meals, the pancreas has to release more insulin to do the same job, fat tends to accumulate around the liver and the abdomen, and inflammatory markers creep up. Over years, that drift is the path to prediabetes, type 2 diabetes, and a cluster of cardiometabolic risk factors.
When insulin sensitivity goes up, that drift reverses. Post-meal glucose excursions get smaller. The same diet produces less metabolic load. Body composition tends to shift. Energy through the afternoon tends to feel steadier because the glucose roller-coaster flattens.
For people who are training mostly for body composition or for staying off medications later in life, this is the bedrock outcome. Strength, VO2 max, and weight loss are downstream of metabolic health. If the underlying muscle is responsive to insulin, almost every other goal gets easier. If it isn't, every goal fights an uphill grade.
How Exercise Builds Insulin Sensitivity in Practice
Three things drive the chronic adaptation, and they layer on top of each other.
First, contracting muscle takes up glucose without insulin. Muscle contraction activates AMP-activated protein kinase (AMPK), which signals GLUT4 vesicles to translocate to the cell membrane. Once GLUT4 is at the membrane, glucose flows into the muscle cell down its concentration gradient. This pathway is independent of insulin, which is why exercise lowers blood glucose even in people whose insulin signaling is impaired. It is also why walking after meals works so well. The contractions pull glucose out of the bloodstream while you are still absorbing the meal.
Second, training increases GLUT4 protein content in the muscle. The Croymans 2013 trial showed this directly in resistance-trained subjects, and dozens of aerobic-training trials show the same effect. More GLUT4 means more glucose-uptake capacity per unit of muscle. The structural change persists as long as training continues.
Third, training builds more muscle. Skeletal muscle is the biggest glucose-disposal tissue in the body. Adding 5 pounds of metabolically active muscle expands the total glucose sink, which lowers the insulin needed to handle a given meal. This is one of the reasons strength training after 60 is so high-value. The muscle you keep is the buffer against age-related metabolic decline.
Aerobic training, resistance training, and breaking up sitting all hit these mechanisms, just through different doors. Aerobic work hits the AMPK pathway hard and improves mitochondrial density (which makes the muscle better at burning the glucose it imports). Resistance work expands the muscle and raises its GLUT4 content. Sitting breaks add daily contractions in a population that often skips both of the other two. They stack.
Get an evidence-based plan built for you
FitCraft, our mobile fitness app, pairs you with an AI coach who builds you a personalized plan around your goals, schedule, and fitness level. Every FitCraft program is designed by Domenic Angelino, MPH (Brown University) and NSCA-CSCS, with research published in the Journal of Strength and Conditioning Research and Medicine & Science in Sports & Exercise.
Take the Free Assessment Free • 2 minutes • No credit cardCombined Training Tends to Win
If you want to maximize the insulin-sensitivity gain per week of training, the evidence points to combining aerobic and resistance work rather than picking one. Cuff and colleagues (2003) in Diabetes Care ran one of the cleaner head-to-head trials. Twenty-eight postmenopausal women with type 2 diabetes were randomized to 16 weeks of aerobic training only, aerobic plus resistance training, or a non-exercise control. Glucose disposal (a clamp-measured gold-standard of insulin sensitivity) improved significantly more in the combined-training group than in the aerobic-only group.
The mechanism story makes sense of this. Aerobic training is the high-AMPK stimulus and the mitochondrial-density stimulus. Resistance training is the muscle-and-GLUT4 stimulus. They do different jobs. A program that does both stacks two non-overlapping adaptations onto the same muscle.
That said, the floor is high. Either modality alone works, and the right protocol is the one you will actually do consistently. Pick one, get a habit, then add the other. A six-month aerobic-only block followed by adding resistance is better than a "comprehensive" plan you abandon in week 4.
Common Misconceptions
Misconception 1: "I only need to exercise on the weekend to fix my metabolism."
The acute effect of a single bout fades within 24 to 48 hours. A single Saturday workout buys you better insulin sensitivity through Sunday and probably part of Monday. By Wednesday it is essentially gone. To keep the benefit at baseline, you need to overlap bouts, which in practice means 3 to 4 sessions a week minimum, ideally with a couple of days having any activity at all. Frequency matters more than total weekly minutes for this specific outcome.
Misconception 2: "Cardio is the diabetes exercise. Lifting is just for muscle size."
Croymans 2013 and a long line of subsequent trials are clear that resistance training is a high-impact intervention for insulin sensitivity in its own right. The mechanism is partly acute (every set activates AMPK and GLUT4) and partly structural (more muscle, more GLUT4 per cell). Major bodies like the American Diabetes Association now include resistance training in their exercise recommendations for type 2 diabetes specifically because the evidence is strong. If you can only do one mode, do whichever you will do. If you can do both, do both.
Misconception 3: "I do an intense workout every day, so a desk job doesn't matter."
The Dunstan 2012 result is robust. Sitting for 5 hours straight produces a measurably worse postprandial glucose and insulin response than the same 5 hours broken up with short walks, even after controlling for total daily exercise. The acute training effect doesn't fully insulate you against the metabolic load of long uninterrupted sitting. A daily workout is a separate input from how you spend the other 23 hours. Both matter.
What the Research Suggests Going Forward
Step back from the individual studies and the message is unusually clean. Exercise improves insulin sensitivity on an acute timescale (one bout, 24 to 48 hours of effect), on a chronic timescale (12 weeks of training, structural change in the muscle), and on a daily-living timescale (breaking up sitting, lower postprandial spikes). Aerobic, resistance, and combined modalities all work, with combined approaches winning the head-to-head trials. The mechanism is well-characterized down to the protein level.
Two honest limitations. First, most chronic-training trials run 12 to 24 weeks. Whether the gains observed at 24 weeks scale linearly out to year 5 is inferred, not directly demonstrated. Second, individual responsiveness varies. A subset of people in any training study are "low responders" whose insulin sensitivity moves less than the group average. The reasons are not fully understood and likely include genetics, sleep, baseline diet, and stress.
The practical forward picture is straightforward. Aim for 3 to 4 sessions per week of structured training, ideally including both aerobic and resistance work. Break up sitting through the day with short walks, especially after meals. Don't try to substitute one for the other. Stacking the acute effect, the chronic adaptation, and the daily-living interruptions is what produces a metabolism that ages well.
References
- Bird SR, Hawley JA. "Update on the effects of physical activity on insulin sensitivity in humans." BMJ Open Sport & Exercise Medicine 2.1 (2017): e000143. doi:10.1136/bmjsem-2016-000143
- Way KL, Hackett DA, Baker MK, Johnson NA. "The Effect of Regular Exercise on Insulin Sensitivity in Type 2 Diabetes Mellitus: A Systematic Review and Meta-Analysis." Diabetes & Metabolism Journal 40.4 (2016): 253-271. doi:10.4093/dmj.2016.40.4.253
- Croymans DM, Paparisto E, Lee MM, Brandt N, Le BK, Lohan D, Lee CC, Roberts CK. "Resistance training improves indices of muscle insulin sensitivity and beta-cell function in overweight/obese, sedentary young men." Journal of Applied Physiology 115.9 (2013): 1245-1253. doi:10.1152/japplphysiol.00485.2013
- Dunstan DW, Kingwell BA, Larsen R, Healy GN, Cerin E, Hamilton MT, Shaw JE, Bertovic DA, Zimmet PZ, Salmon J, Owen N. "Breaking up prolonged sitting reduces postprandial glucose and insulin responses." Diabetes Care 35.5 (2012): 976-983. doi:10.2337/dc11-1931
- Cuff DJ, Meneilly GS, Martin A, Ignaszewski A, Tildesley HD, Frohlich JJ. "Effective exercise modality to reduce insulin resistance in women with type 2 diabetes." Diabetes Care 26.11 (2003): 2977-2982. doi:10.2337/diacare.26.11.2977

Frequently Asked Questions
How quickly does exercise improve insulin sensitivity?
A single bout of moderate or vigorous exercise improves whole-body insulin sensitivity within hours, and the effect persists for roughly 24 to 48 hours. Bird and Hawley (BMJ Open Sport & Exercise Medicine, 2017) summarized the acute-versus-chronic literature and concluded that repeated bouts compound into longer-lasting adaptations through GLUT4 expression and mitochondrial changes. The practical implication is that you cannot bank insulin sensitivity across a week with one Saturday workout. Frequency matters.
Is aerobic exercise or resistance training better for insulin sensitivity?
Both work, and the combination tends to beat either alone. Cuff et al. (Diabetes Care, 2003) found combined aerobic-plus-resistance training improved insulin sensitivity more than aerobic training alone in postmenopausal women with type 2 diabetes. Croymans et al. (Journal of Applied Physiology, 2013) showed pure resistance training raised muscle GLUT4 protein and oral indices of muscle insulin sensitivity in sedentary young men. Pick what you will actually do consistently, then add the other modality once the first is a habit.
Does HIIT improve insulin sensitivity more than steady-state cardio?
Per unit of time, yes. Bird and Hawley (2017) reviewed the dose-response data and reported that higher intensities produce larger gains in insulin action for a matched time investment. But continuous moderate-intensity training works fine when total weekly volume is matched. The right protocol is the one you will adhere to, since the chronic effect depends on doing the work week after week.
How much does training improve insulin sensitivity in type 2 diabetes?
Way et al. (Diabetes & Metabolism Journal, 2016) pooled randomized controlled trials in adults with type 2 diabetes and found a pooled effect size of -0.588 (95% CI -0.816 to -0.359) for insulin resistance reduction. That is a moderate-to-large effect, comparable to many first-line medications. The benefit appeared with both aerobic and resistance protocols and tended to be larger with longer interventions.
Can breaking up sitting really change insulin sensitivity?
Yes. Dunstan et al. (Diabetes Care, 2012) had overweight and obese adults sit for 5 hours straight, or interrupt the sitting every 20 minutes with a 2-minute walk break. The walking-break condition cut postprandial insulin by 23% and postprandial glucose by 24%. Short, frequent movement breaks recruit leg muscle to clear glucose without insulin, taking pressure off the pancreas through the rest of the day.