- Normal adult cadence is 100 to 120 steps per minute. Most healthy adults sit around 110. Brisk walking pushes it to 120 to 130.
- Normal stride length is about 1.4 meters (step length around 70 cm). Both scale with leg length, so taller people naturally cover more ground per step at the same cadence.
- Comfortable walking speed is 1.2 to 1.4 m/s (about 2.7 to 3.1 mph). Bohannon and Williams (2011), in Physiotherapy, pooled 41 studies and gave the canonical reference values.
- Walking speed predicts survival in older adults. Studenski et al. (2011), in JAMA, pooled 34,485 older adults and found every 0.1 m/s of usual walking speed tracked with a 12 percent lower risk of death.
- The signs of an abnormal gait are asymmetry, instability, and change from your baseline. Limping, shortened stride on one side, shuffling, widened stance, or a visible hip drop are the patterns worth flagging.
"Is there something wrong with my gait?" lands on r/exercisescience every couple of months, usually attached to a clip someone took of themselves walking. The replies range from "your hips are uneven, see a PT immediately" to "looks fine, stop overthinking it." Both are usually wrong. A normal walking gait has measurable parameters that the research has nailed down across decades, and most of the things that look "off" in a phone clip are either camera angle artifacts or minor asymmetries that everyone has.
This piece walks through what a clinically normal walking gait actually looks like (the phases, the cadence, the stride length, the speed), and then the patterns that actually suggest something is worth looking at. The good news is that the basics of gait analysis are simple enough that you can do a useful self-assessment with a phone camera and a measuring tape. The harder news is that some of the signs of an off gait are subtle, and a few of them do warrant a clinical visit.
Here is the plan. We will cover the gait cycle itself (the two phases every leg goes through). We will hit the three measurable parameters: cadence, stride length, and speed. We will look at what the research says about gait speed and longevity. We will close with the actual signs of an abnormal gait and what to do about them.
The Gait Cycle: Stance and Swing
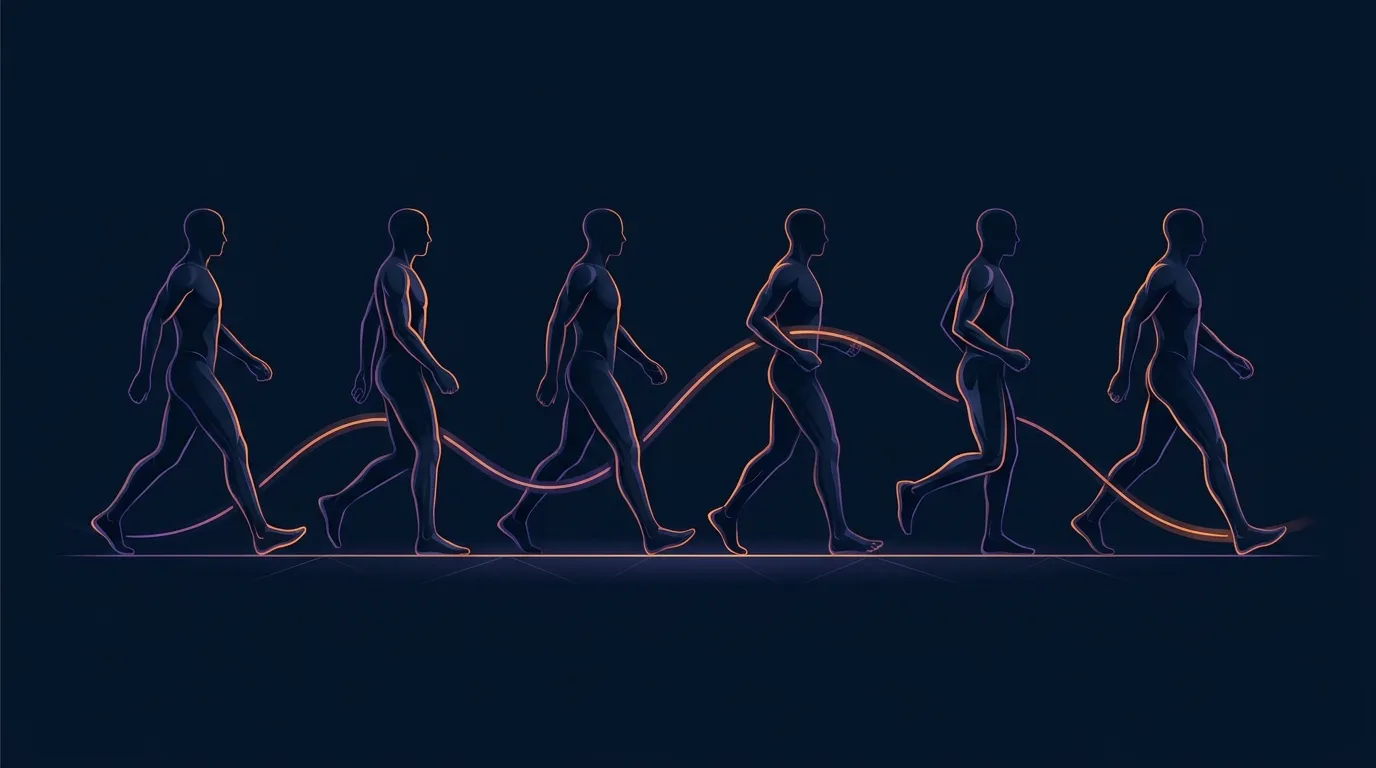
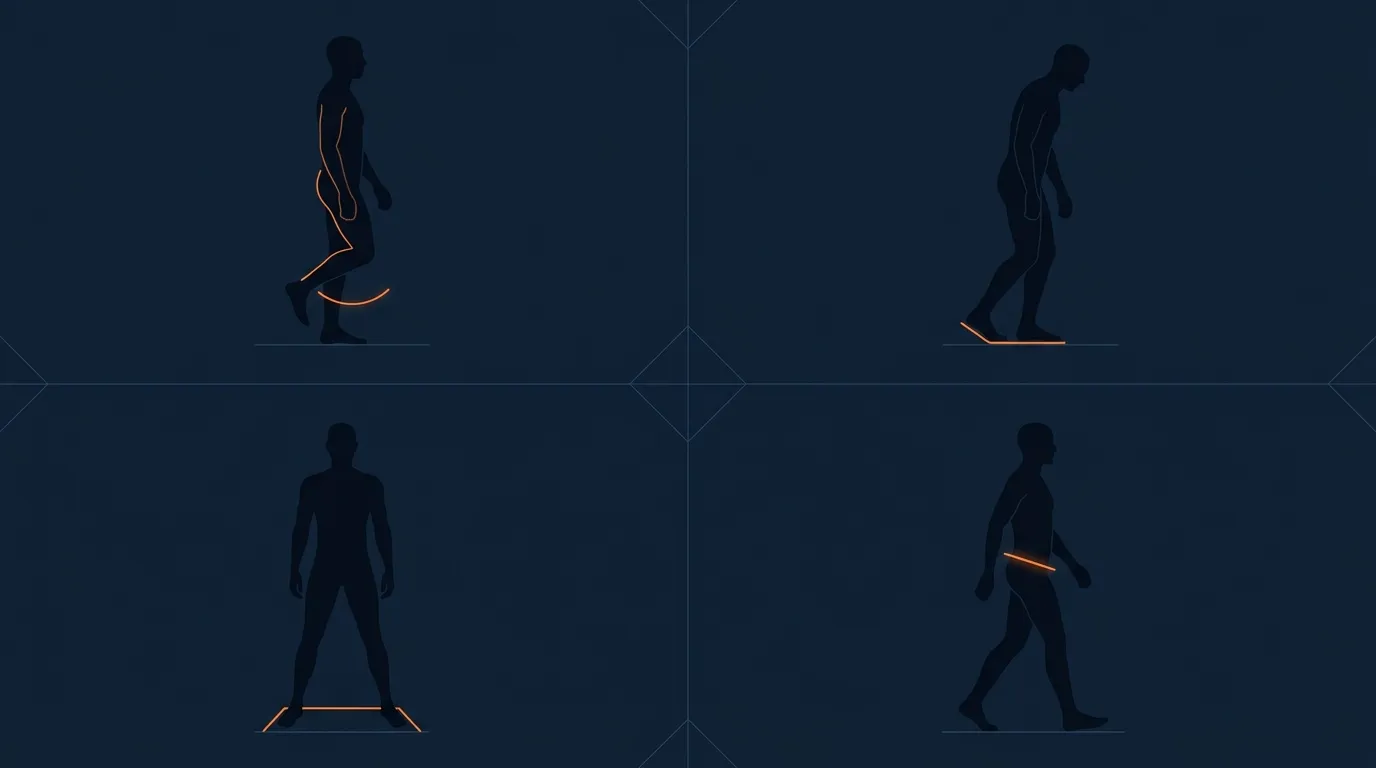
One full gait cycle for a single leg starts when one foot strikes the ground and ends when that same foot strikes the ground again. The cycle splits into two phases. Stance phase, when the foot is on the ground supporting body weight, runs about 60 to 62 percent of the cycle. Swing phase, when the foot is in the air moving forward to the next strike, runs about 38 to 40 percent. There is a brief overlap (about 10 percent of the cycle on each end of stance) when both feet are on the ground, called double support.
Stance phase breaks down further into recognizable sub-phases. Initial contact is the heel strike, where the heel hits the ground first in a normal gait. Loading response transfers body weight onto the limb. Midstance is the body passing over the supporting foot. Terminal stance is the heel lifting as you prepare to push off. Pre-swing is the toe-off, where the toes leave the ground and the leg starts to swing forward. Swing phase has its own three sub-phases (initial, mid, and terminal swing) that bring the foot forward and prepare it for the next heel strike.
Why this matters: a clinically normal gait is identifiable by the smooth, predictable flow through these phases. The most common gait abnormalities show up as a disruption to a specific phase. Antalgic gait shortens stance on the painful side (the body unloads the limb as quickly as possible). Foot drop disrupts swing phase (the toes hit the ground because the foot can't dorsiflex). Trendelenburg gait disrupts midstance (the hip drops because the gluteus medius can't stabilize the pelvis). The vocabulary is technical but it makes pattern recognition possible.
The Three Numbers: Cadence, Stride, Speed
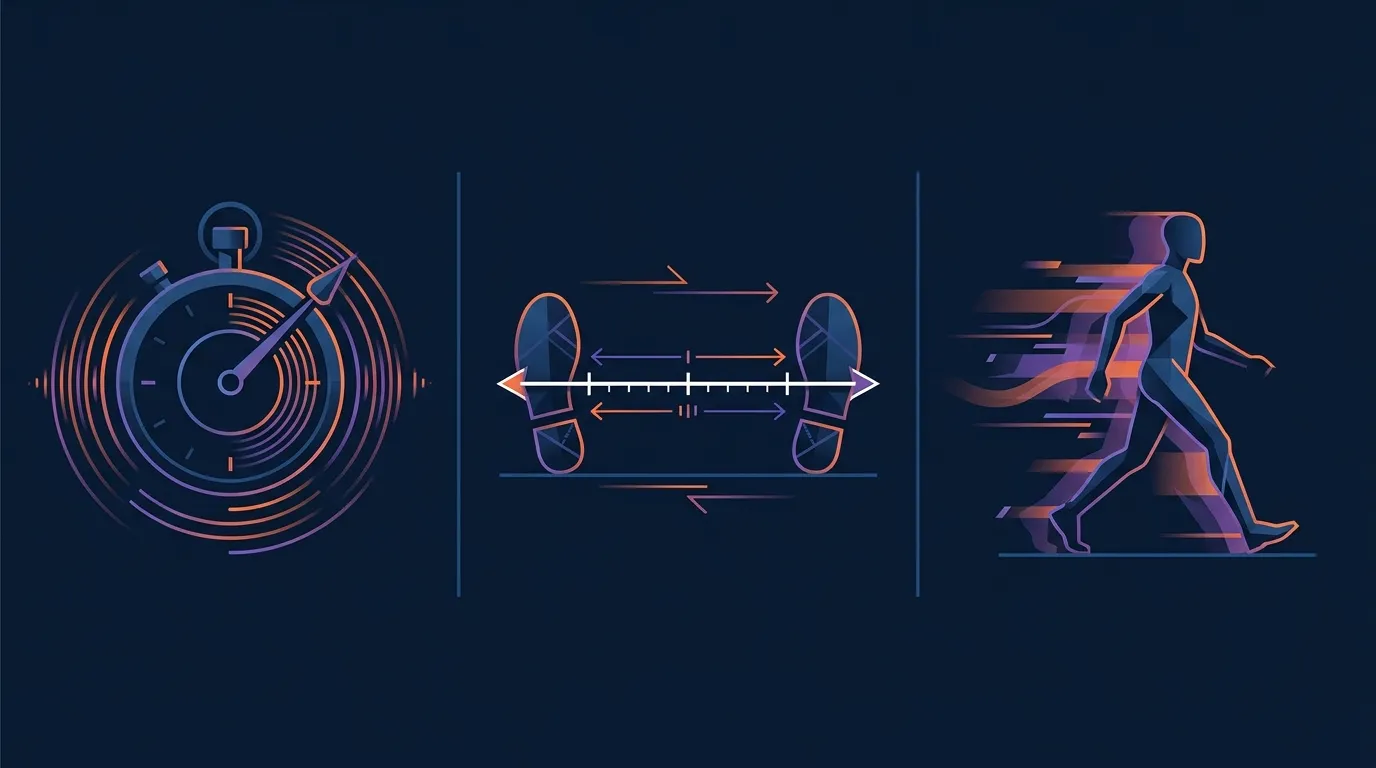
You can describe most of a walking gait with three measurements. Each one is easy to take. Together they cover roughly 80 percent of what a clinical gait assessment quantifies.
Cadence. Steps per minute. Normal adult cadence is 100 to 120 steps per minute, with most healthy adults landing around 110. Brisk walking sits at 120 to 130. Race walking and very slow walking sit outside that range. To measure your own: count your steps for 30 seconds while walking at a comfortable pace, then double it. Any phone step tracker will also give you cadence estimates for any walk, and the trend over months is more informative than any single number.
Stride length. The distance from one heel strike to the next heel strike of the same foot. Average for healthy adults is about 1.4 to 1.5 meters, or roughly 55 to 60 inches. Step length (one heel strike to the opposite heel strike, half of stride length) is around 70 to 75 cm. Both scale with leg length, so taller people naturally have longer strides at the same cadence. To measure: walk normally across a known distance and divide by the number of strides.
Walking speed. Distance covered per unit time. The canonical reference is Bohannon and Williams (2011) in Physiotherapy. They pooled gait-speed data across 41 studies and reported normal comfortable walking speed for healthy adults at 1.2 to 1.4 meters per second (about 2.7 to 3.1 mph), with maximum walking speeds in the 1.8 to 2.0 m/s range. Speed declines with age, but a slow walking speed in mid-life is more often a fitness signal than an age signal.
Gait Speed and Longevity
The clinical reason gait speed matters is one of the cleaner findings in the longevity literature. Studenski and colleagues (2011), in JAMA, pooled individual-participant data from 9 cohort studies covering 34,485 older adults. Every 0.1 meters per second of usual walking speed tracked with a 12 percent lower risk of death. Gait speeds at or above 1.0 m/s in adults aged 65 and older tracked with above-average life expectancy. Speeds at or above 1.2 m/s tracked with exceptional life expectancy. Gait speed alone predicted survival as accurately as multivariable models that included age, sex, mobility-aid use, and self-reported function.
That is not because walking fast causes longevity directly. Gait speed is an integrator. It picks up cardiovascular fitness, lower-body strength, balance, neurological function, joint health, vision, and cognition simultaneously. When several of those decline, gait speed falls before the individual symptoms become obvious. That is why slowing walking speed in mid-life is taken seriously in geriatric practice. It is a leading indicator, not just a symptom.
For the deeper dive on this evidence, see our pieces on walking speed as a longevity marker and the sit-to-stand test for functional aging. The walking-speed measure is the more accessible of the two, and a 10-meter walk test you do once a year is a reasonable home version.
Knowing what to do is the easy part.
FitCraft, our mobile fitness app, pairs you with an AI coach who builds you a personalized plan around your goals, schedule, and fitness level. Every FitCraft program is designed by Domenic Angelino, MPH (Brown University) and NSCA-CSCS, with research published in the Journal of Strength and Conditioning Research and Medicine & Science in Sports & Exercise.
Take the Free Assessment Free • 2 minutes • No credit cardSigns of an Abnormal Gait
The most useful indicators are asymmetry, instability, and changes from your previous baseline. None of them are catastrophes on their own. All of them are worth a closer look if they are new or progressing.
Limping or favoring one leg. The classic antalgic gait. The painful or weak side spends less time in stance. Stride length is usually shorter on the unaffected side because the affected leg can't fully push off. Most common causes are hip, knee, or ankle pain; less common but more concerning are neurological deficits. Acute limping after an injury is mechanical and usually self-limiting. Persistent limping with no clear injury history needs an evaluation.
Arms not swinging symmetrically. Normal walking has reciprocal arm swing. Each arm swings forward as the opposite leg swings forward. A reduced or absent arm swing on one side is one of the earliest signs of Parkinson's disease and can also signal a previous stroke or shoulder pathology.
Shortened stride on one side. Stride length should be roughly symmetric, give or take a couple of centimeters. A consistent difference of more than 10 percent between sides is worth investigating. The most common causes are leg-length differences, hip flexor tightness, or compensation for joint pain.
Widened stance. Healthy walking has a step width (the lateral distance between feet) of about 5 to 13 cm. A noticeably wider stance is a balance compensation. The body widens its base of support because it does not trust the narrower one. This shows up with peripheral neuropathy, cerebellar dysfunction, and after vestibular conditions.
Shuffling or foot-dragging. Reduced foot clearance during swing phase. Common in Parkinson's, normal-pressure hydrocephalus, and certain spinal conditions. Mild scuffing of one shoe is sometimes just biomechanical wear; consistent shuffling of both feet is not normal and warrants evaluation.
Toe-walking or flat-footed strike. Normal walking is heel-toe. A persistent flat-foot strike or toe-walk in an adult often signals an Achilles or calf issue, foot drop (no heel strike because dorsiflexion is weak), or a chronic compensation pattern. Children who toe-walk after age 3 should be evaluated for tight Achilles or developmental conditions.
Visible hip drop on each step. The Trendelenburg pattern. The hip on the swing side drops below the level of the stance side because the gluteus medius on the stance side is too weak to hold the pelvis level. Trendelenburg is one of the few gait abnormalities you can usually fix with a focused glute-strengthening program. Side-lying hip abduction, clamshells, and single-leg step-ups are the standard prescriptions.
What to Do About a Gait That Looks Off
The first useful question is whether the gait has actually changed or you are just noticing it for the first time. Watch an older video of yourself walking if you have one. Compare. Asymmetries that have been there for years and are not associated with pain are usually individual variation, not pathology. Bodies are not symmetric. Walking gaits are not symmetric.
If the gait has changed, the second question is what changed alongside it. New pain, new weakness, new numbness or tingling, a recent injury, recent medication changes (statins, blood pressure medications, and some antidepressants can affect gait), or any combination of those all push toward a clinical evaluation. Family physicians and physical therapists are the right starting points. Neurology referral is appropriate if the changes are bilateral, progressive, and not associated with a mechanical cause.
If the gait change is mechanical (new pain, identifiable injury, gradual decline in fitness), the boring answer is also the right one: build the muscle and the cardiovascular fitness back up. Walking gait is a reflection of underlying strength, balance, and endurance. Bodyweight strength work, balance practice, and consistent daily walking will improve gait parameters in months. Our piece on staying functionally fit over 60 covers the strength-and-balance fundamentals that matter most for gait preservation.
If you want to track your own gait at home, the cheapest useful protocol is a 10-meter walk test once a month. Measure 10 meters along a flat hallway. Walk at your normal comfortable pace from a flying start (start walking a couple of meters before the start line so you are already at steady pace). Time how long it takes you to cover the 10 meters. Speed equals 10 divided by the seconds. Healthy adults should comfortably hit 1.2 m/s or better. A consistent slowdown over months is a real signal. Pair it with a step counter to see cadence trends, and you have a useful home gait monitor.
Frequently Asked Questions
What is a normal walking gait?
A normal adult walking gait is a smooth, symmetrical, two-phase cycle. Each leg spends about 60 percent of the cycle in stance and 40 percent in swing. Cadence runs roughly 100 to 120 steps per minute. Step length is around 70 cm and stride length (one full cycle for one leg) is around 1.4 meters. Comfortable walking speed for healthy adults sits between 1.2 and 1.4 meters per second, per the Bohannon and Williams (2011) meta-analysis in Physiotherapy. The pattern that makes a gait normal is even cadence, symmetric stride, minimal lateral sway, and a heel-to-toe foot strike that flows into a clean push-off.
What is a normal walking gait called?
Clinically it is called a heel-toe gait or a reciprocal gait. Reciprocal means the arms and legs swing in opposite pairs (right arm forward with left leg, left arm forward with right leg). Heel-toe describes the foot strike: the heel makes initial contact, the foot rolls through the midfoot, and the big toe pushes off. The cycle has two main phases for each foot, stance (60 percent) and swing (40 percent), with brief periods of double support. This is the gait that develops in healthy children by about age 7 and stays remarkably stable through adulthood until disease or injury changes it.
What is a normal walking stride length?
Average stride length for healthy adults is about 1.4 to 1.5 meters (around 55 to 60 inches), measured heel-strike to heel-strike of the same foot. Step length, the distance from one heel-strike to the opposite heel-strike, is around 70 to 75 cm (about 28 to 30 inches). Both numbers scale with leg length, so taller people naturally have longer strides at the same cadence. Stride length shortens with age, with fatigue, and with most neurological conditions that affect gait. A noticeably shortened or asymmetric stride is one of the most common early signs of a gait problem.
What is a normal walking cadence?
Normal adult walking cadence runs 100 to 120 steps per minute, with most healthy adults landing around 110. Brisk walking pushes cadence up to 120 to 130. Cadence is one of the easiest gait variables to measure: count steps for 30 seconds and double it. It is one of the most stable parameters. Substantial drops in cadence over months or years often track with declining fitness, joint pain, or early neurological changes. A simple step-tracker on a phone will give you a cadence estimate for any walk, and trends over time are more informative than any single number.
What are signs of an abnormal gait?
The most useful indicators are asymmetry, instability, and changes from your baseline. Limping or favoring one leg, arms not swinging symmetrically, a shortened stride on one side, a widened stance, shuffling or foot-dragging, toe-walking or a flat-footed strike instead of heel-toe, difficulty starting or turning, and a visible lateral hip drop (Trendelenburg pattern) are the patterns worth flagging. Any of these as a new development warrants a clinical evaluation. Studenski et al. (2011) in JAMA found that adults aged 65+ losing more than 0.1 m/s of usual walking speed over a year is a clinically meaningful change worth flagging to a physician.