Walk into any gym. Look at the floor. You'll see them lined up like sad little logs: foam rollers, lacrosse balls, vibrating massage sticks, knobby peanut things. Someone is grimacing on top of one right now, breathing through their teeth, convinced they are "releasing fascia."
Foam rolling has become one of those things you do because everyone does it. The trainer says roll your IT band. The yoga instructor says roll your glutes. Your knee hurts? Roll your quads. Your back hurts? Roll your back. The advice is everywhere. The evidence is more interesting.
The good news: foam rolling actually works. The honest news: it works less than fitness culture claims, and probably not for the reasons you've been told.
This article walks through what 21 randomized studies pooled in a 2019 meta-analysis actually found about foam rolling for performance and recovery. We'll also cover what foam rolling probably does mechanistically (spoiler: not fascia), how long you should roll, when in your workout, and what to do if you're rolling daily and feel like nothing is changing.
The Study: Wiewelhove et al. (2019) and Why It Matters
The most rigorous synthesis of the foam rolling literature is a 2019 meta-analysis by Wiewelhove and colleagues, published in Frontiers in Physiology. The researchers searched four databases, screened more than 1,800 records, and ultimately included 21 randomized studies with a combined sample of about 357 healthy adults.
Each study compared foam rolling (or a similar self-myofascial release device like a roller stick) to a passive control. The outcomes covered both sides of the rolling-out narrative: performance markers (sprint speed, vertical jump, strength, flexibility) and recovery markers (perceived muscle soreness, performance restoration after fatigue).
What They Found Before Exercise
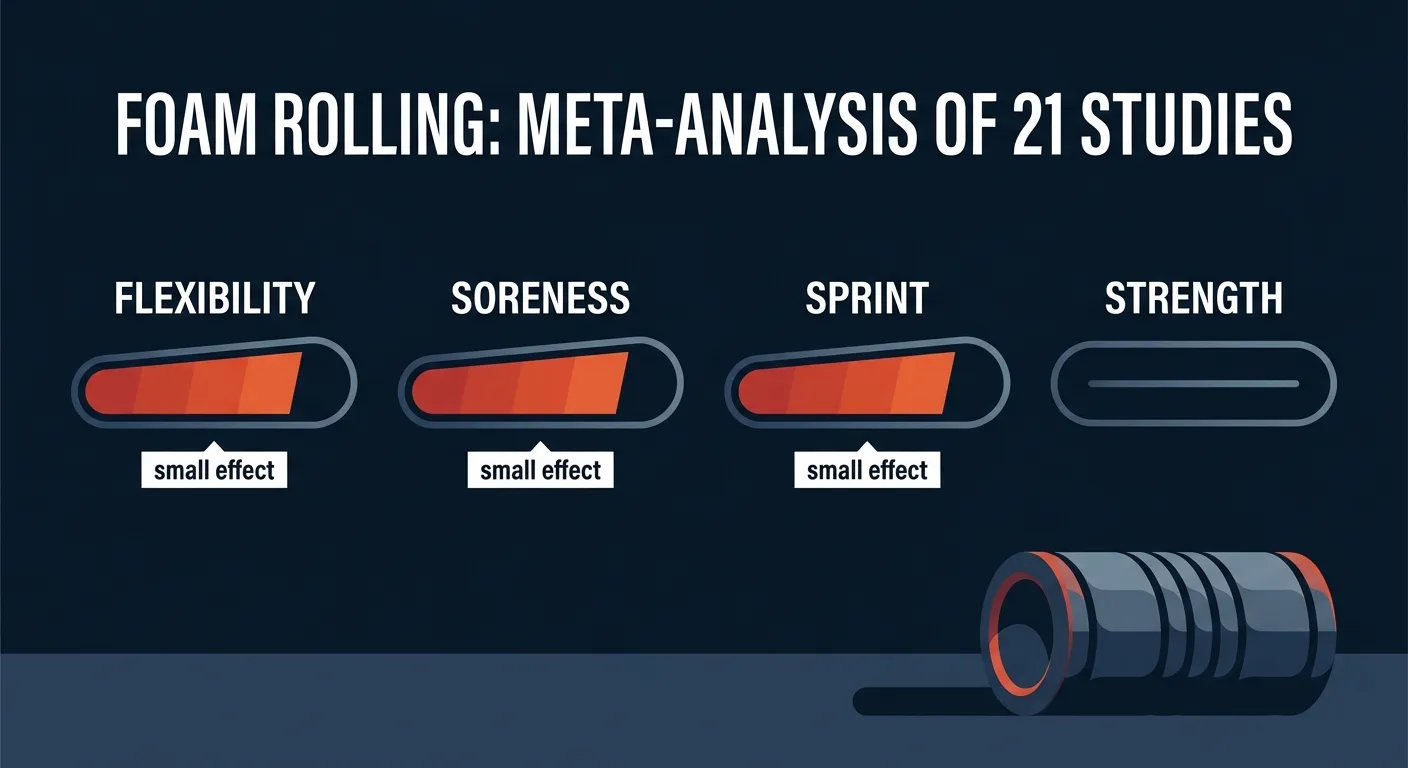
When foam rolling was used before a workout as a warm-up tool, the meta-analysis found:
- Sprint performance: small but significant improvement (Cohen's d = 0.32). Rolling appears to give a small acute boost to short-duration speed efforts.
- Flexibility: small to moderate improvement in range of motion immediately after rolling. The effect appears within minutes and dissipates over the next 10 to 20 minutes.
- Maximum strength: no meaningful effect. Foam rolling neither helped nor hurt 1-rep max or maximal voluntary contraction.
- Vertical jump: no meaningful effect on jumping power.
This last point is actually useful. Long-duration static stretching (60+ seconds per muscle) is known to acutely reduce strength and power output. Foam rolling appears to give you the flexibility benefit of stretching without that strength cost. If you want to loosen up your hamstrings before squats without losing pop in your legs, rolling beats stretching.
What They Found After Exercise
When foam rolling was used after a workout for recovery, the meta-analysis reported:
- Muscle soreness: small but consistent reduction in perceived DOMS over the following 24 to 72 hours.
- Sprint performance recovery: small improvement, helping people regain speed after fatiguing exercise.
- Strength recovery: small benefit, though less consistent across studies.
- Vertical jump recovery: small benefit, again, less consistent.
Pearcey et al. (2015) in the Journal of Athletic Training ran one of the cleanest studies inside this body of literature. After a bout of 10 sets of 10 back squats at 60% 1RM, participants who foam rolled for 20 minutes immediately, 24 hours, and 48 hours after the workout reported less muscle soreness, sprinted faster, jumped higher, and maintained better strength than a no-rolling control. The dose was deliberate, and the benefit was visible. But the participants were university-aged athletes doing a brutal eccentric protocol; the effect on a recreational lifter doing three sets of moderate squats is going to be smaller.
The key takeaway from both the meta-analysis and Pearcey's individual study: foam rolling helps. The help is modest. It is not nothing.
Why Foam Rolling Probably Does Not "Release Fascia"
Most foam rolling instruction starts with some version of "we're going to release the fascia." This is almost certainly wrong, and the people doing the rolling deserve a better story.
Behm and Wilke (2019), writing in Sports Medicine, reviewed the proposed mechanisms of self-myofascial release and concluded that mechanical deformation of fascia is implausible under normal foam rolling conditions. Fascia is dense, sheet-like connective tissue with tensile strength approaching that of tendon. The forces required to permanently change its shape are on the order of those used in surgical interventions, not the 30 to 60 kg of bodyweight a person applies through a piece of foam.
So what is happening when rolling feels like it's working?
- Pain modulation. Sustained pressure on a sore muscle triggers descending inhibition in the central nervous system. The brain turns down its pain signal. This is the same mechanism that explains why pressing hard on a stubbed toe feels relieving.
- Transient reduction in muscle tone. Rolling appears to briefly reduce neural drive to a muscle, allowing it to relax. This is why a tight hamstring lengthens after rolling but the effect fades within 10 to 20 minutes.
- Increased blood flow. Local circulation increases under and around the rolled tissue. This may explain the small recovery effect.
- Diffuse noxious inhibitory control. A fancy term for "discomfort in one area can mute discomfort everywhere." Rolling out one quad can briefly raise the pain threshold across the whole body.
None of these mechanisms involve permanently lengthening connective tissue. All of them are real, measurable, and useful. The fascia narrative is just a marketing-friendly story attached to a set of actual neurophysiological effects.
Why does this matter? Because if you understand the mechanism, you understand the dose. You don't need to roll until the fascia "lets go" (it won't). You need to roll long enough to trigger the neural response (usually 30 to 120 seconds per area), and then move on.
How Long to Roll and How Often
The systematic review by Cheatham, Kolber, Cain, and Lee (2015) in the International Journal of Sports Physical Therapy pulled together the dose-response evidence available at the time. The pattern that emerged across studies was simple: most of the benefit shows up within 30 to 120 seconds per muscle group, and additional time produces diminishing returns.
Hughes and Ramer (2019) extended this in a duration-focused systematic review in the International Journal of Sports Physical Therapy and reached a similar conclusion: rolling durations under 90 seconds per muscle were generally sufficient for acute range-of-motion gains. There is no compelling evidence that ten-minute marathons on a single muscle outperform the standard one to two minutes.
A reasonable evidence-based protocol:
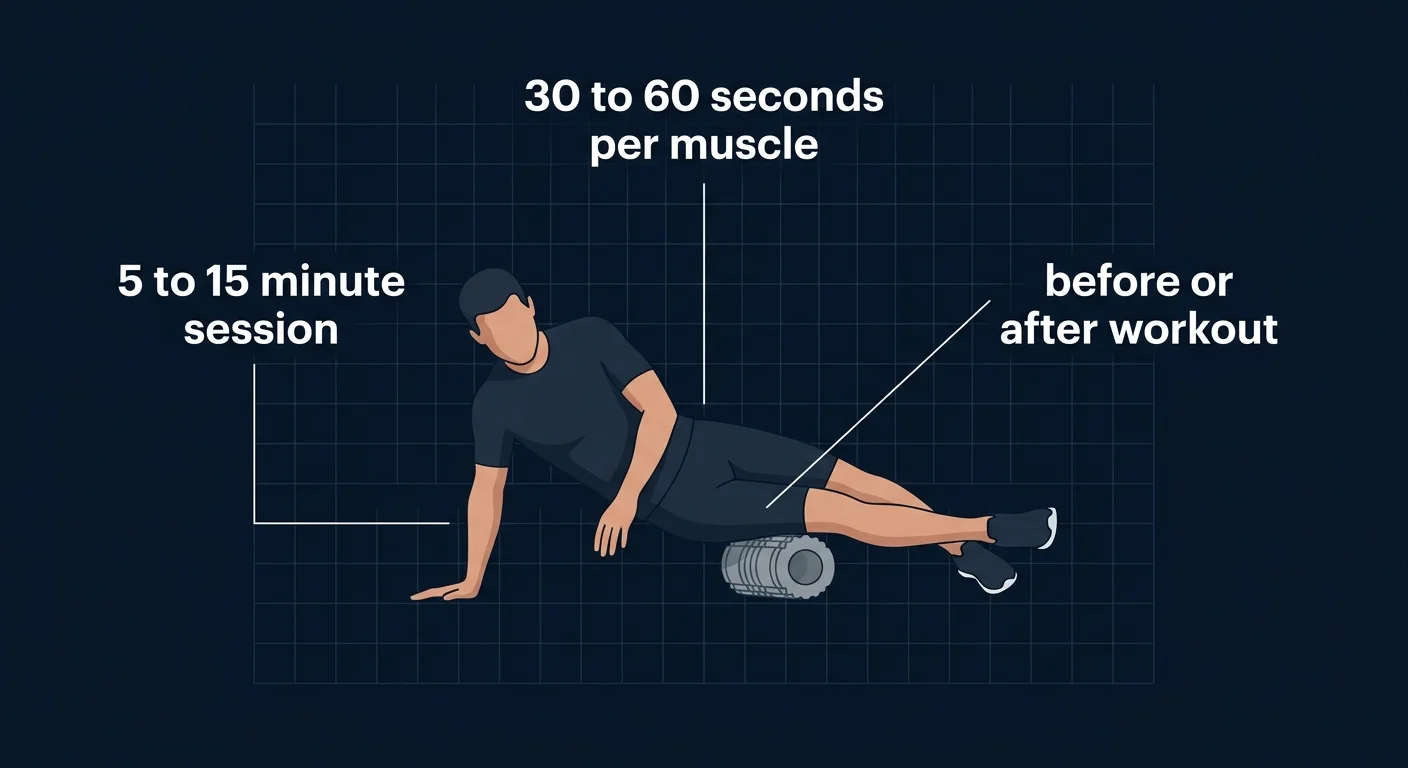
- Per muscle group: 30 to 60 seconds of slow rolling, then 30 seconds of focused pressure on the most tender spots.
- Total session: 5 to 15 minutes covering the muscles relevant to the work you just did or are about to do.
- Frequency: daily is fine and appears safe; the marginal benefit beyond 3 to 4 times per week is small.
- Pressure: uncomfortable but not unbearable. If you cannot breathe normally or hold the position for 30 seconds, you're rolling too aggressively.
Get an evidence-based plan built for you
FitCraft, our mobile fitness app, pairs you with an AI coach who builds you a personalized plan around your goals, schedule, and fitness level. Every FitCraft program is designed by Domenic Angelino, MPH (Brown University) and NSCA-CSCS, with research published in the Journal of Strength and Conditioning Research and Medicine & Science in Sports & Exercise.
Take the Free Assessment Free • 2 minutes • No credit cardFoam Rolling vs. Stretching, Massage, and Active Recovery
Rolling does not exist in a vacuum. It competes for your limited recovery time with stretching, massage, light movement, and sleep. Where does it actually rank?
Versus static stretching: for acute range-of-motion gains, both work. Hendricks et al. (2020) summarized the relevant trials and noted that foam rolling produced flexibility increases comparable to static stretching without the acute reductions in strength and power that follow long static holds. If you want to loosen up before lifting, rolling is the safer bet.
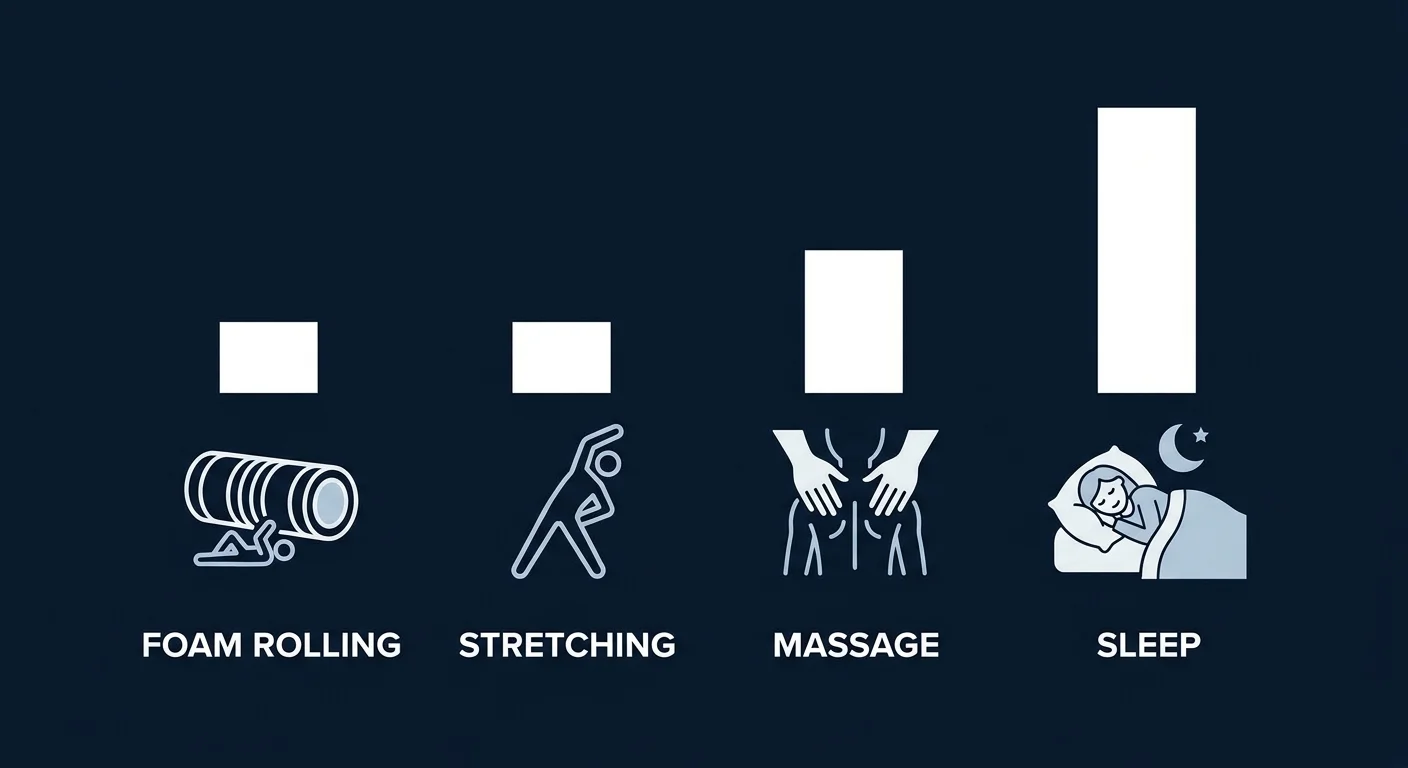
Versus massage: hands-on massage from a trained therapist produces larger and more consistent recovery effects than foam rolling, particularly for DOMS reduction. This shows up in the broader recovery literature: in the 99-study meta-analysis covered in our active recovery research piece, massage was the single highest-ranked recovery technique. Foam rolling appears to capture some, but not all, of those benefits at a fraction of the cost.
Versus active recovery: light cardio between hard training days is sometimes prescribed for recovery, but the meta-analytic evidence is weak. Foam rolling has slightly better data for reducing perceived soreness than light jogging or cycling, though both effects are small. Pick whichever fits your routine.
Versus sleep: not even close. Adequate sleep is the foundation of recovery; everything else, including rolling, is a small percentage on top. If you are rolling religiously and sleeping six hours, you are optimizing in the wrong order.
Common Misconceptions About Foam Rolling
Misconception 1: "Rolling the IT band will fix knee pain"
The iliotibial band is one of the toughest connective tissues in the body. It does not stretch, and it does not "release" under foam roller pressure. What rolling the lateral thigh does is provide pressure-based pain modulation on the muscles that attach to and around the IT band: the tensor fasciae latae, vastus lateralis, and gluteus maximus. That can transiently reduce discomfort. It will not change the IT band itself. If you have lateral knee pain, address the root cause (usually weak hip abductors, training-load progression, or running mechanics), not the symptom.
Misconception 2: "It should hurt to work"
The "pain equals gain" framing is wrong here. The neural effects of foam rolling appear at moderate pressures, not maximal ones. Rolling so hard that you brace, hold your breath, or twitch away from the roller is more likely to trigger a protective response than a relaxation one. Aim for a 5 to 7 out of 10 discomfort. If it's a 9, back off.
Misconception 3: "More is better"
Spending 30 minutes per day rolling each muscle group is not supported by the research. The dose-response curve flattens quickly. Two minutes per muscle group, two to four days per week, captures most of the benefit visible in the literature. The diminishing-returns shape is similar to what shows up in the rest periods between sets research: past a sensible threshold, more time spent doesn't translate to more outcome.
Misconception 4: "Foam rolling lengthens muscles permanently"
It doesn't. The range-of-motion improvements from a rolling session last roughly 10 to 30 minutes and then return to baseline. Long-term flexibility gains require regular stretching or training the joint through a full range of motion under load. Rolling can be a useful warm-up to make those positions feel easier; it does not replace them.
Who Foam Rolling Actually Helps Most
The benefits show up most clearly in three populations:
People doing eccentric or unaccustomed training. If you just did your first squat workout in two months, or you ran downhill for the first time this year, the muscle damage and resulting DOMS are exactly what foam rolling has the strongest data for reducing.
People with limited range of motion before a workout. Tight hips before squats. Tight thoracic spine before overhead pressing. Rolling can transiently improve the position you'll need to train in, without the strength-blunting effects of long static stretching.
Athletes in a sport with repeated short sprints. The pre-exercise sprint benefit (d = 0.32 in the Wiewelhove meta-analysis) is small but real. For team-sport athletes whose performance hinges on repeated short bursts, that's worth the five minutes.
Who it helps least: people looking for a passive solution to a structural problem. Chronic low back pain from poor hip mobility, weak glutes, and 50 hours of sitting per week is not going to be fixed by foam rolling. Rolling can be part of a plan; it cannot be the plan.
What the Research Suggests Going Forward
The current state of the evidence is interesting precisely because it's neither a slam dunk nor a debunk. Foam rolling does something. It does it via mechanisms other than the ones marketed. The effects are small. They are also free, low-risk, and available to anyone with $20 and a piece of foam.
Limitations worth flagging:
- Most studies are short. The bulk of the evidence is acute (single session) or subacute (a few days). The long-term effects of habitual rolling on flexibility, soreness, and performance are less well-studied.
- Most studies used trained or recreationally active participants. The transferability to older adults, people in pain rehab, or sedentary beginners is less established.
- "Foam rolling" is not standardized. Studies vary in duration, pressure, roller density, and which muscles get rolled. The 21 studies in Wiewelhove's meta-analysis used protocols ranging from 30 seconds to 2 minutes per muscle, with very different rollers.
- Placebo and expectation effects are hard to control. You can't blind someone to whether they're foam rolling. Some of the perceived soreness reductions probably reflect expectation.
None of these caveats invalidate the headline finding. They just suggest that "I rolled and felt better" is genuine, modest, and not magic. Use rolling as a small, repeatable tool inside a broader recovery and training plan. If your recovery picture is dominated by chronic under-sleeping and over-volume, the answer is sleep more and train less (a pattern explored in our overtraining syndrome research writeup), not roll harder.
How FitCraft Treats Recovery
Most fitness apps treat recovery as something you figure out on your own. They give you the workouts and assume you'll work out the rest. That's a problem, because the difference between training programs that progress and programs that stall often comes down to whether recovery is built into the structure or treated as an afterthought.
FitCraft's approach is to program recovery as part of the plan. Your AI coach lays out training days and rest days based on the program you're working through, rather than dropping you into a calendar of workouts and leaving the rest day decisions to your gut feeling. Programs include yoga and mobility sessions when they fit the goal, and the underlying training-stress logic adjusts as you progress.
Foam rolling, if you like it, fits well as a small layer on top of that structure. Roll out tight hips before a strength day. Roll your quads and calves after a hard cardio block. Don't expect the rolling to replace the rest day. The rest day is the bigger lever.
References
- Wiewelhove T, Döweling A, Schneider C, Hottenrott L, Meyer T, Kellmann M, Pfeiffer M, Ferrauti A. "A Meta-Analysis of the Effects of Foam Rolling on Performance and Recovery." Frontiers in Physiology. 2019;10:376. doi:10.3389/fphys.2019.00376
- Pearcey GE, Bradbury-Squires DJ, Kawamoto JE, Drinkwater EJ, Behm DG, Button DC. "Foam rolling for delayed-onset muscle soreness and recovery of dynamic performance measures." Journal of Athletic Training. 2015;50(1):5-13. doi:10.4085/1062-6050-50.1.01
- Hendricks S, Hill H, Hollander SD, Lombard W, Parker R. "Effects of foam rolling on performance and recovery: A systematic review of the literature to guide practitioners on the use of foam rolling." Journal of Bodywork and Movement Therapies. 2020;24(2):151-174. doi:10.1016/j.jbmt.2019.10.019
- Cheatham SW, Kolber MJ, Cain M, Lee M. "The effects of self-myofascial release using a foam roll or roller massager on joint range of motion, muscle recovery, and performance: a systematic review." International Journal of Sports Physical Therapy. 2015;10(6):827-838. PMC4637917
- Behm DG, Wilke J. "Do Self-Myofascial Release Devices Release Myofascia? Rolling Mechanisms: A Narrative Review." Sports Medicine. 2019;49(8):1173-1181. doi:10.1007/s40279-019-01149-y
Frequently Asked Questions
Does foam rolling actually work?
Yes, but the effects are smaller than fitness culture claims. A 2019 meta-analysis of 21 studies in Frontiers in Physiology by Wiewelhove et al. found that foam rolling before exercise produced a small but significant improvement in sprint performance and flexibility, and foam rolling after exercise produced a small reduction in soreness and a small benefit to performance recovery. The effects are real, but the effect sizes are mostly small (Cohen's d under 0.4). Foam rolling is a useful tool, not a miracle.
Does foam rolling reduce muscle soreness?
Modestly. Pearcey et al. (2015) in the Journal of Athletic Training found that 20 minutes of foam rolling immediately after a workout and again 24 and 48 hours later reduced perceived muscle soreness and helped preserve sprint and power performance versus a no-rolling control. The Wiewelhove 2019 meta-analysis confirmed a small but consistent effect on post-exercise soreness. Foam rolling will not eliminate DOMS, but it can take the edge off.
How long should you foam roll for?
Most studies showing benefit used 30 to 120 seconds per muscle group, repeated for two to four sets. Hughes and Ramer's 2019 systematic review found that durations under 90 seconds per muscle were generally sufficient for acute flexibility gains, and adding more time produced diminishing returns. For post-workout recovery, total sessions of 10 to 20 minutes appear to capture most of the benefit.
Should you foam roll before or after a workout?
Both have evidence, but the use case differs. Foam rolling before training can transiently improve range of motion and may slightly improve sprint performance without the strength-reducing effects seen with long static stretching. Foam rolling after training appears to reduce soreness over the next 48 to 72 hours. The Wiewelhove meta-analysis found small benefits in both contexts. Pick the one that fits your routine; do not feel obligated to do both.
Does foam rolling release fascia?
Probably not in the way the term implies. Behm and Wilke (2019) in Sports Medicine reviewed the proposed mechanisms and concluded that mechanical fascial release is unlikely to occur during foam rolling because fascia is far too tough to deform with hand pressure or bodyweight. The more plausible mechanisms are neurophysiological: changes in pain perception via descending inhibition, transient reductions in muscle tone, and improved blood flow. The benefits are real even if the fascia story is not.