You've probably seen it on fitness Instagram. Someone posts about "overtraining symptoms" alongside a list of vague complaints, tired, sore, unmotivated, not making gains. The comments fill up with people convinced they've been pushing too hard. The solution? Deload weeks, adaptogens, recovery protocols that cost more than a gym membership.
Here's the thing: most people who think they're overtrained aren't even close. True overtraining syndrome is a serious clinical condition that can sideline elite athletes for months or years. It's been studied by some of the biggest names in sports science and sports medicine. And the consensus from that research tells a very different story than what you'll find on TikTok.
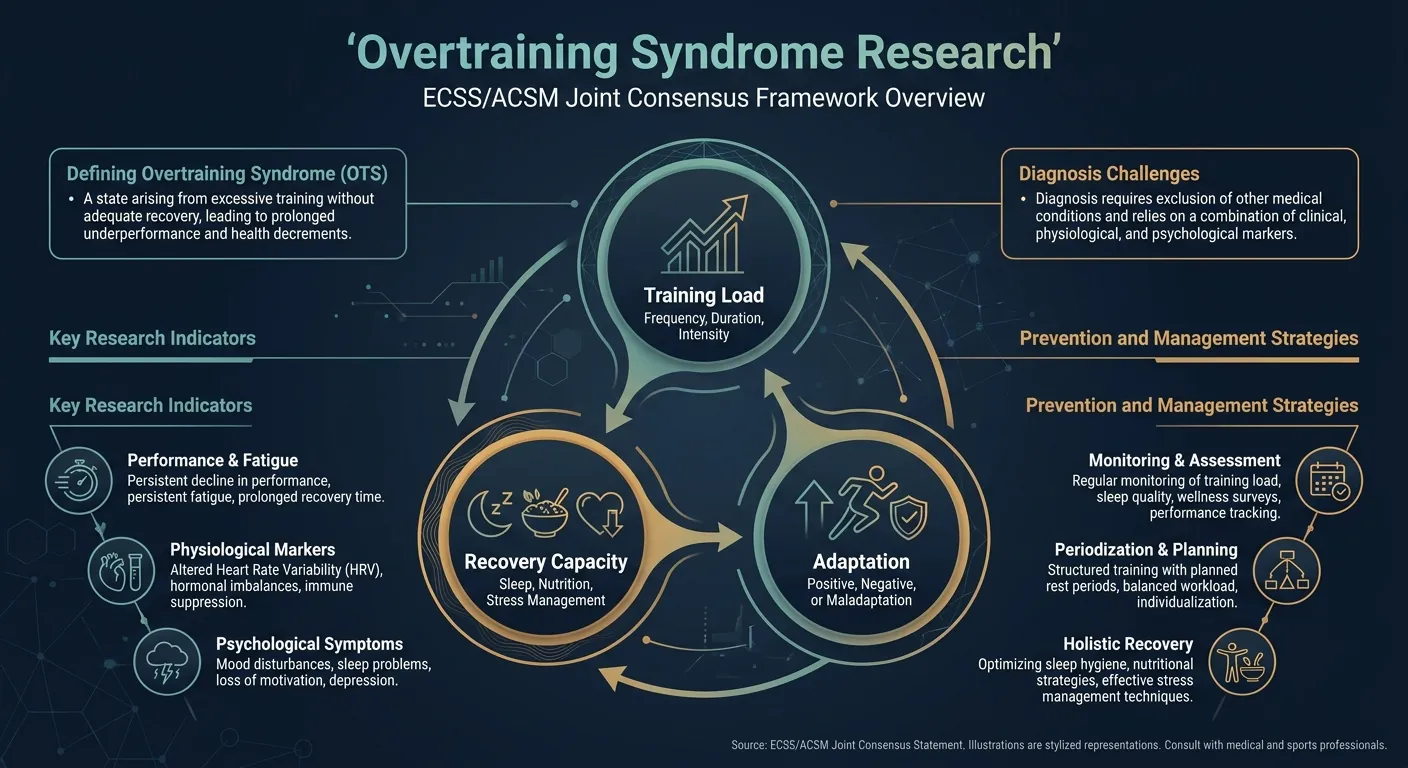
In 2013, the European College of Sport Science (ECSS) and the American College of Sports Medicine (ACSM) published a joint consensus statement. The most comprehensive expert agreement on overtraining ever produced. Let's break down what they actually found, what it means for regular people who exercise, and why understanding this spectrum matters more than any single biomarker.
What Are the Three Stages of Overtraining?
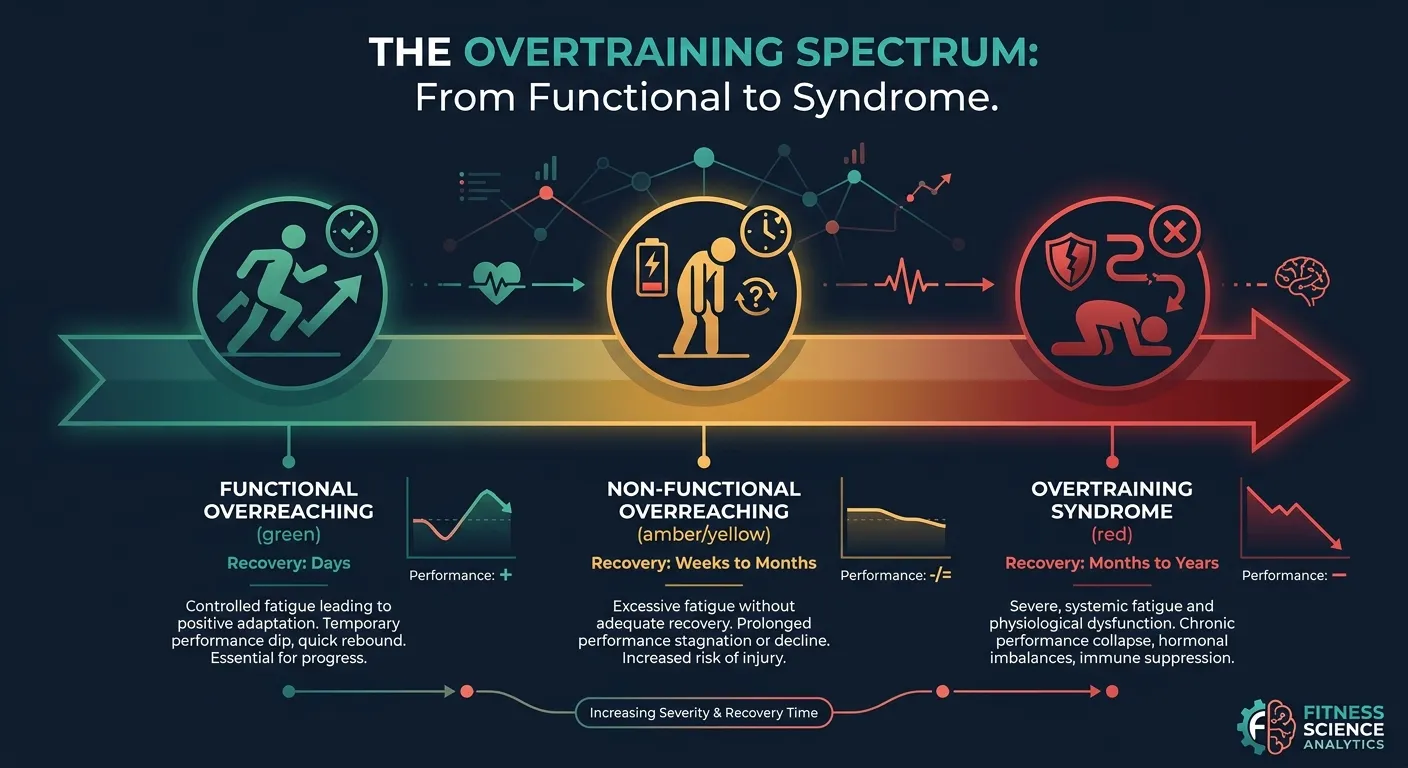
Overtraining is a continuum with three stages: functional overreaching (a planned dip that you recover from in days), non-functional overreaching (an unplanned slump lasting weeks to months), and true overtraining syndrome (performance decline that persists for months to years). The difference between them is recovery time.
| Stage | Recovery Time | Outcome |
|---|---|---|
| Functional overreaching (FOR) | Days to ~2 weeks | Supercompensation: you come back stronger |
| Non-functional overreaching (NFOR) | Weeks to months | Stalled performance, no fitness payoff |
| Overtraining syndrome (OTS) | Months to years | Multisystem disorder, sidelines even elite athletes |
One of the most important contributions of the Meeusen et al. (2013) consensus was establishing clear terminology. Before this paper, "overtraining" was used loosely to describe everything from feeling tired after a tough week to career-ending burnout in Olympic athletes. That imprecision made the problem worse. It scared casual exercisers away from training hard enough to make progress.
The consensus established three distinct stages on a continuum:
Functional Overreaching (FOR): The Good Kind
This is the one that's actually supposed to happen. Functional overreaching is a deliberate, short-term performance dip caused by an increase in training load. You push harder than normal for a few days or a week. You feel fatigued. Your performance temporarily drops. Then you rest, and you come back stronger than before. A process called supercompensation.
Every well-designed training program uses functional overreaching. It's the mechanism behind progressive overload. Recovery takes days to roughly two weeks, and the payoff is improved fitness. If you've ever had a brutal training week followed by a lighter week where you suddenly felt like a machine, that's FOR doing exactly what it should.
Non-Functional Overreaching (NFOR): The Warning Sign
This is where things go sideways. Non-functional overreaching happens when you accumulate too much training stress without enough recovery, and instead of bouncing back stronger, your performance stays depressed for weeks to months. The "non-functional" part means you don't get the supercompensation payoff. You just dig a hole.
Symptoms are broader than just feeling tired. Research shows more than 70% of athletes with NFOR self-report emotional disturbances, decreased motivation, irritability, anxiety, difficulty concentrating. Sleep quality often tanks. Training feels disproportionately hard relative to the actual load. You're doing workouts that should be manageable and they're crushing you.
NFOR is recoverable with adequate rest. But "adequate" can mean weeks to months of substantially reduced training, not just a couple of easy days.
Overtraining Syndrome (OTS): The Months-to-Years Problem
True overtraining syndrome is NFOR's bigger, meaner sibling. Performance decrements persist for months to years, even with complete rest (Kreher & Schwartz, 2012). It's a multisystem disorder involving neurological, endocrine, and immunological disruptions. It doesn't just affect your workouts. It affects your mood, sleep, appetite, immune function, and hormonal regulation.
Here's the critical insight from the consensus: you can only distinguish NFOR from OTS in retrospect. At the time someone is experiencing it, the symptoms look identical. The difference is how long recovery takes. If performance comes back in a few weeks, it was NFOR. If it takes six months or a year? That's OTS. This makes early intervention essential, because once you're in OTS territory, there's no shortcut out.
Can Blood Tests Detect Overtraining?
No single blood test reliably detects overtraining. A 2017 systematic review of 38 studies found that resting hormone levels, including the cortisol-to-testosterone ratio, are mostly normal in overtrained athletes. Blood work is useful for ruling out other conditions, not for confirming overtraining.
If you've ever Googled "am I overtrained," you've probably encountered advice about checking your cortisol-to-testosterone ratio. It sounds scientific. It sounds actionable. And according to the research, it's mostly useless for detecting overtraining.
Cadegiani and Kater published a systematic review in 2017 examining every study that measured hormonal markers in overtrained athletes. They analyzed 38 studies total. Their conclusion was remarkably clear: basal levels of hormones, including cortisol, testosterone, and their ratio, were mostly normal in athletes with OTS, NFOR, and FOR compared to healthy athletes.
The only hormonal differences showed up in stimulation tests, not resting bloodwork. When overtrained athletes did maximal exercise tests, their growth hormone (GH) and ACTH responses were blunted, meaning their endocrine system didn't ramp up the way it should during intense effort. But plasma catecholamines and cortisol showed conflicting findings even under stimulation. Other hormonal markers responded normally.
What this means in practice: getting your testosterone and cortisol checked at a lab won't tell you if you're overtrained. It might tell you about other conditions, thyroid issues, clinical hypogonadism, adrenal disorders, which is actually valuable, because those conditions also cause fatigue and performance decline. But as an overtraining diagnostic tool? The science doesn't support it.
It's a Diagnosis of Exclusion
The Meeusen et al. consensus was explicit on this point: overtraining syndrome is diagnosed by ruling everything else out first. Before a doctor can say "this is OTS," they need to exclude anemia, thyroid dysfunction, viral infections, mood disorders, nutritional deficiencies, and a long list of other medical conditions that produce similar symptoms.
This matters because a lot of what people attribute to overtraining actually has a different, and more treatable, cause. Low iron? That'll tank your performance and energy. Subclinical hypothyroid? Same. Depression? Absolutely. Poor sleep quality from stress? That alone can explain most "overtraining" symptoms in recreational exercisers.
How Common Is Overtraining, Really?
True overtraining syndrome is rare in recreational exercisers. Seasonal incidence in elite athletes runs 7 to 20 percent, and lifetime prevalence in elite distance runners approaches 60 percent. For someone training 3 to 5 times a week, it is vanishingly unlikely. Here's where the gap between perception and reality gets wide.
Among elite endurance athletes, seasonal incidence of OTS ranges from 7% to 20% (Kreher & Schwartz, 2012). Lifetime prevalence in elite distance runners approaches 60%. These are people training 15-30+ hours per week, often at high intensity, for years. The volume and chronicity of their training creates genuine overtraining risk.
Among recreational exercisers, people doing 3-5 sessions per week of strength training, running, or app-based workouts, true overtraining syndrome is extremely rare. Not "uncommon." Rare. You're far more likely to be under-training than overtraining.
That doesn't mean you can't feel terrible after a hard training block. You absolutely can. But there's a massive difference between "I pushed hard this week and I'm tired" and a clinical condition that takes months of complete rest to resolve. Confusing the two leads to either unnecessary deloading (leaving gains on the table) or, worse, ignoring an actual medical issue because you've convinced yourself it's just overtraining.
What's Actually Going On When You Feel "Overtrained"
If true OTS is rare in regular exercisers, then what explains the fatigue, the stalled progress, the feeling that everything is harder than it should be?
Usually it's one or more of these, and none of them are overtraining:
- Under-recovery, not over-training. You're sleeping 6 hours instead of 7-8. You're not eating enough protein or total calories. You're chronically dehydrated. The training load itself might be fine, but your body doesn't have the raw materials to adapt to it.
- Life stress compounding training stress. Your body doesn't distinguish between work stress, relationship stress, financial stress, and training stress. They all draw from the same recovery pool. A moderately hard training program becomes unmanageable when you're also dealing with a newborn, a job crisis, or a move.
- Monotonous programming. Doing the same exercises, same rep schemes, same intensity week after week doesn't cause overtraining, but it does cause psychological burnout and motivation collapse. You're not overtrained. You're bored.
- Poor program design. Too much intensity, not enough variation in stimulus, no periodization, no deload structure. A static program that doesn't adapt to your current state will eventually run you into a wall. Not because the total volume is excessive, but because it's not matched to your recovery capacity on any given day. The deload week research exists precisely to address this: planned volume reductions every 4-6 weeks prevent accumulated fatigue from becoming a real problem.
The consensus statement supports this distinction. Meeusen et al. emphasize that training is not the only stressor, psychological stress, sleep disruption, nutritional inadequacy, and illness all contribute to the overtraining continuum. An athlete doing objectively moderate training volume can develop NFOR if every other recovery factor is compromised.
Enjoying the article?
Start a new fitness routine today, written by me and coached by the AI I designed.
Take the Free Assessment Free • 2 minutes • No credit card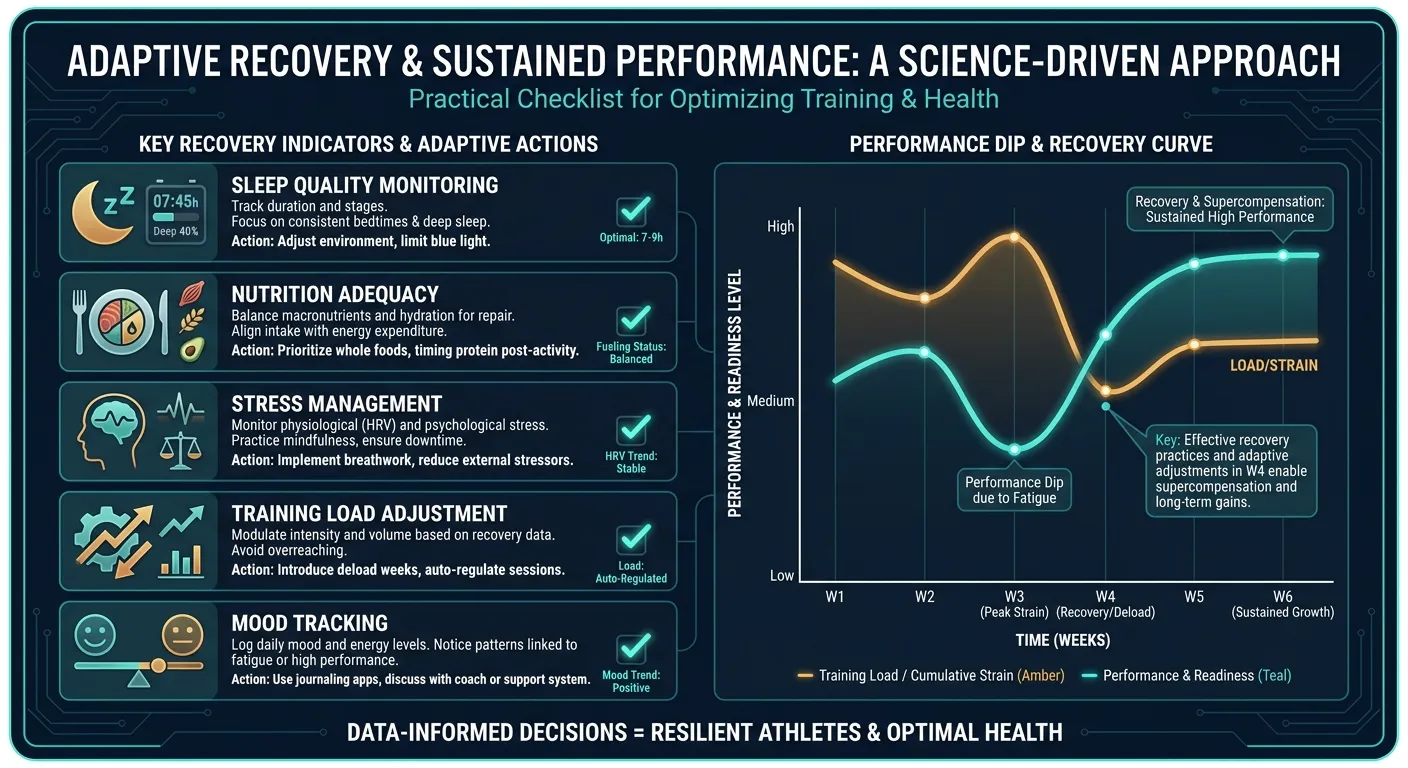
What the Consensus Actually Recommends for Prevention
The ECSS/ACSM statement doesn't just define the problem. It outlines prevention strategies. And they're surprisingly straightforward:
Individualize Training Load
One-size-fits-all programs are a risk factor. What's an appropriate training stimulus for an experienced athlete is excessive for a beginner. What's manageable in a low-stress week becomes too much during finals or a work deadline. The consensus emphasizes that training load must be adjusted to the individual, their fitness level, their recovery capacity, and their current life context.
This is where most fitness apps fail. A static 12-week program doesn't know you slept four hours last night. It doesn't know you're fighting a cold. It gives you Tuesday's workout regardless of whether Tuesday's workout makes sense for the state you're actually in.
Monitor Mood and Subjective Fatigue
Since objective biomarkers are unreliable, the consensus highlights subjective monitoring as one of the best early warning systems. Mood disturbances, especially decreased motivation, increased irritability, and perceived exertion that doesn't match the actual workload, are among the most consistent early indicators of overreaching.
More than 70% of athletes with NFOR and OTS self-reported emotional changes before their performance visibly declined. They felt something was off before the numbers confirmed it. The practical takeaway: if training has felt disproportionately hard for more than a week or two, and your motivation has cratered, pay attention. That's not laziness. That's signal.
Periodize Recovery, Not Just Training
Periodization usually refers to structuring training phases, building volume, peaking intensity, then recovering. But the consensus emphasizes that recovery itself needs to be periodized. Deload weeks aren't optional. Sleep isn't negotiable. Nutrition must match training demands. These aren't nice-to-haves. They're the infrastructure that determines whether your training stimulus produces adaptation or damage.
How Adaptive AI Addresses the Overtraining Problem
The consensus statement's core recommendation, individualize training load in real time, is exactly the problem that adaptive AI coaching was built to solve.
FitCraft's 3D AI trainer, Ty, doesn't just give you a predetermined workout and hope for the best. Ty adjusts volume, intensity, and exercise selection based on how you're actually performing. If movements that were easy last week suddenly feel heavy, the session scales back. If you're crushing it, the challenge scales up. This isn't a gimmick, it's the training load management approach that the research says prevents overreaching from becoming non-functional.
Here's what that looks like in practice:
- Automatic volume adjustment, If your performance metrics dip, Ty reduces the session's total work. No ego-driven push through a rigid program.
- Built-in recovery periods, The programming includes periodized lighter sessions, not as an afterthought but as a structural feature of the training plan.
- Variety by design, Strength, mobility, yoga, cardio, and dynamic movement rotate through your plan. Monotony, one of the psychological precursors to burnout, is engineered out.
- Progressive overload without reckless escalation, Difficulty increases when the data supports it, not on an arbitrary weekly schedule.
FitCraft includes this adaptive programming as a core feature. Training that adjusts to your actual recovery state is, according to the research, the single most important factor in preventing overreaching from spiraling into something worse.
Common Misconceptions About Overtraining
Misconception: "If I'm sore and tired, I'm overtrained"
Soreness and fatigue after hard training are normal. They're signs that you gave your body a stimulus it needs to adapt to. Functional overreaching. The productive kind, involves temporary fatigue by definition. The red flags for actual overreaching are: performance that stays depressed for more than two weeks despite adequate rest, persistent mood changes unrelated to obvious life stressors, and training that feels dramatically harder than the load warrants. Feeling tired after leg day doesn't qualify.
Misconception: "My cortisol:testosterone ratio will tell me if I'm overtrained"
This one persists despite the research clearly not supporting it. Cadegiani and Kater's 2017 systematic review of 38 studies found that resting hormonal levels, including this ratio, were mostly normal in overtrained athletes. The fitness industry latched onto this biomarker because it sounds precise and testable. But the science says it's not a reliable indicator. Get bloodwork if you're concerned, just know that normal results don't rule out overreaching, and abnormal results might point to a completely different condition.
Misconception: "Regular gym-goers need to worry about overtraining"
If you're training 3-5 times per week with reasonable volume. The kind of programming most fitness apps deliver, true OTS is vanishingly unlikely. The prevalence data is clear: overtraining syndrome is overwhelmingly a condition of elite and competitive athletes training at extreme volumes for extended periods. For everyone else, the real risk is under-recovering. Fix your sleep, eat enough, manage your stress. That solves 90% of what people blame on overtraining.
What the Research Suggests Going Forward
The overtraining literature has real limitations. Most studies focus on endurance athletes, runners, cyclists, swimmers. There's far less research on overtraining in strength training populations, recreational exercisers, or people following app-based programs. The hormonal research, while informative, hasn't produced a reliable early diagnostic marker. And the fundamental problem remains: you can't distinguish NFOR from OTS until you see how long recovery takes.
What is clear: the solution isn't to train less out of fear. It's to train smarter. Individualized load management, adequate recovery infrastructure, attention to subjective warning signs, and programming that adapts to your current state. Not your state from three weeks ago, are the evidence-based approaches that the consensus supports.
The overtraining scare has probably done more harm than good for average exercisers. It's turned "I'm tired after a hard week" into "I might be overtraining," which leads to unnecessary rest, lost momentum, and, ironically. The kind of engagement decay that makes people quit entirely. If you want to understand what productive hard training followed by planned rest looks like, the active recovery research and the deload week science together give you the full picture. Understanding the actual spectrum helps you push when pushing is productive and pull back when pulling back is warranted.
That's not a message you can build a supplement brand around. But it is what the science says.
References
- Meeusen R, Duclos M, Foster C, Fry A, Gleeson M, Nieman D, Raglin J, Rietjens G, Steinacker J, Urhausen A. "Prevention, diagnosis and treatment of the overtraining syndrome: Joint consensus statement of the European College of Sport Science (ECSS) and the American College of Sports Medicine (ACSM)." European Journal of Sport Science 13.1 (2013): 1-24. doi:10.1080/17461391.2012.730061
- Cadegiani FA, Kater CE. "Hormonal aspects of overtraining syndrome: a systematic review." BMC Sports Science, Medicine and Rehabilitation 9 (2017): 14. doi:10.1186/s13102-017-0079-8
- Kreher JB, Schwartz JB. "Overtraining Syndrome: A Practical Guide." Sports Health 4.2 (2012): 128-138. doi:10.1177/1941738111434406
- Budgett R. "Fatigue and underperformance in athletes: the overtraining syndrome." British Journal of Sports Medicine 32.2 (1998): 107-110. doi:10.1136/bjsm.32.2.107
- Halson SL, Jeukendrup AE. "Does overtraining exist? An analysis of overreaching and overtraining research." Sports Medicine 34.14 (2004): 967-981. doi:10.2165/00007256-200434140-00003
Frequently Asked Questions
What is overtraining syndrome and how is it diagnosed?
Overtraining syndrome (OTS) is a condition of persistent performance decline and fatigue lasting months to years, caused by excessive training without adequate recovery. According to the 2013 ECSS/ACSM joint consensus statement by Meeusen et al., OTS is a diagnosis of exclusion, meaning doctors must first rule out other medical causes like anemia, thyroid dysfunction, or depression before confirming it. There is no single blood test or biomarker that reliably diagnoses overtraining syndrome.
What is the difference between overreaching and overtraining?
Functional overreaching (FOR) is a planned, short-term performance dip lasting days to two weeks that leads to supercompensation and improved fitness. Non-functional overreaching (NFOR) is an unplanned performance decline lasting weeks to months with symptoms like persistent fatigue and mood disturbance. Overtraining syndrome (OTS) involves performance decrements lasting months to years. The key difference is recovery time, and you can only distinguish NFOR from OTS in retrospect.
Can blood tests detect overtraining syndrome?
No single blood test reliably detects overtraining syndrome. A 2017 systematic review by Cadegiani and Kater found that basal hormone levels, including the cortisol-to-testosterone ratio often promoted in fitness media, are mostly normal in overtrained athletes. Only stimulation tests (like maximal exercise tests) showed blunted GH and ACTH responses. Blood work is useful for ruling out other conditions, not for confirming OTS.
How common is overtraining syndrome?
True overtraining syndrome is rare in recreational exercisers. Seasonal incidence in elite athletes ranges from 7-20%, with lifetime prevalence in elite endurance runners approaching 60%. For the average gym-goer doing 3-5 sessions per week, actual OTS is extremely uncommon. Most people who think they're overtrained are actually under-recovered. Not sleeping enough, not eating enough, or stacking life stress on top of training stress.
Does FitCraft help prevent overtraining?
FitCraft's AI coach Ty continuously adjusts workout volume, intensity, and exercise selection based on your actual performance and recovery signals. If you're struggling with movements that were easy last week, Ty scales the session back instead of pushing you through a rigid program. This adaptive approach mirrors what the ECSS/ACSM consensus recommends: individualized training loads with built-in recovery periods. The free version includes this adaptive programming.