For decades, the joint pain, muscle loss, stiff shoulders, and slowly shrinking bones that hit women in their mid-40s and 50s were treated as separate "aging" problems. One doctor for the shoulder. Another for the knee. Vague reassurance about calcium for the bones. Nothing about muscle at all.
A 2024 review in Climacteric changed the framing.
Vonda Wright and colleagues argued the cluster is one thing, tied to one cause, and it deserves a single name: the musculoskeletal syndrome of menopause. The prevalence numbers are not small. Roughly 47 million women worldwide enter the menopause transition each year. About 70 percent of them experience musculoskeletal symptoms, and about a quarter are functionally disabled at some point during the transition. If you are a woman in your 40s reading this, the odds are just under three in four that you will feel this cluster in some form.
This article walks through what the syndrome actually includes, what the mechanistic story tells us about why it happens, what the strongest exercise trial shows about reversing pieces of it, and what the evidence says about hormone therapy for the joint-pain component.
The Wright Framing: One Syndrome, Not Five Complaints
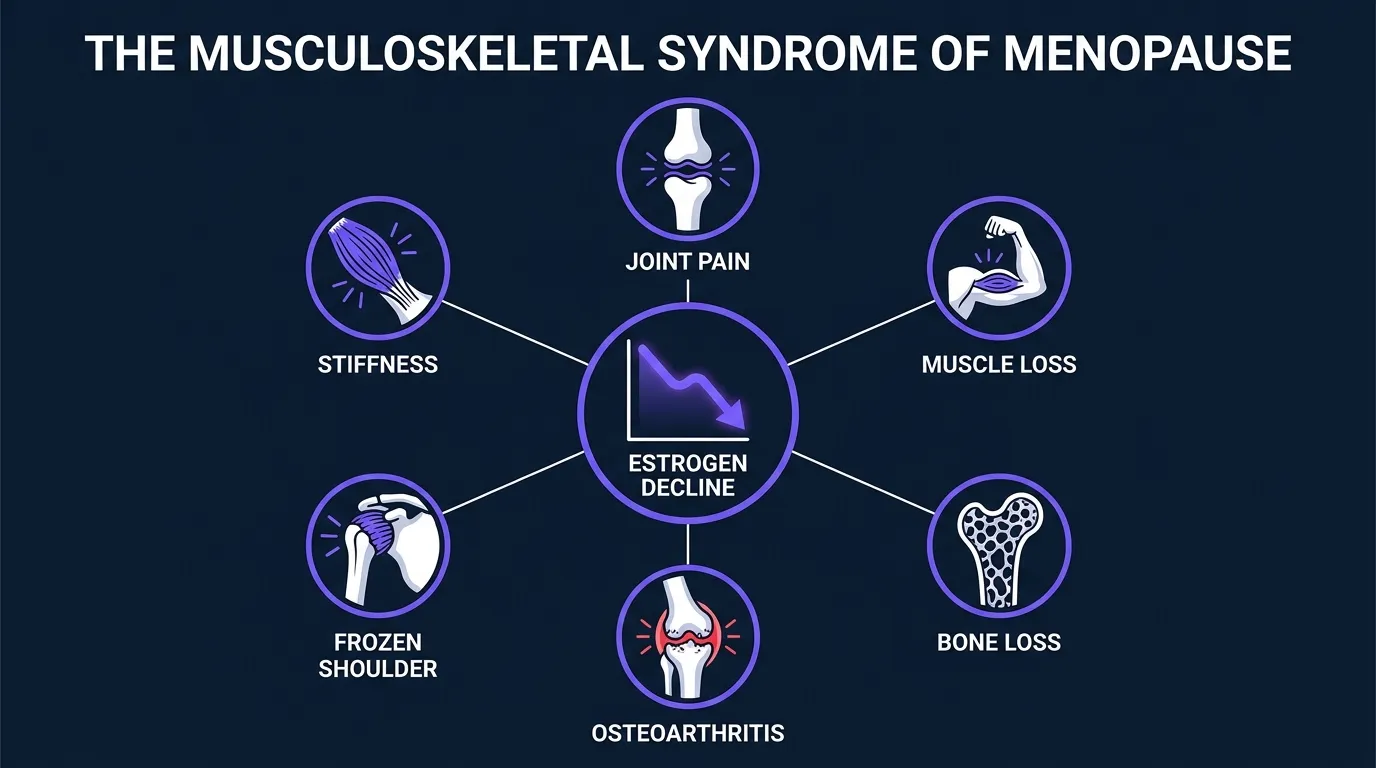
The Wright et al. (2024) review in Climacteric is a clinical narrative review, not a randomized trial. What it did was aggregate the mechanistic and clinical literature and propose that the menopause-related musculoskeletal picture should be treated as a coherent syndrome. The abstract names the core cluster explicitly (arthralgia, loss of muscle mass, loss of bone density, and progression of osteoarthritis), and the review discusses several closely related components in the same clinical picture:
- Arthralgia: joint pain, often bilateral and without a clear mechanical cause. Hands, knees, and shoulders are the common sites. Wright cites literature putting arthralgia prevalence in perimenopausal women at over 50 percent.
- Sarcopenia: loss of muscle mass, muscle quality, and muscle strength. The rate of loss accelerates in the perimenopausal window and continues post-menopause.
- Loss of bone mineral density: the well-known part. Bone loss accelerates sharply in the first few years around the final menstrual period and continues at a slower rate afterward.
- Progression of osteoarthritis: not just wear-and-tear, but an estrogen-modulated process. Cartilage tissue has estrogen receptors, and degradation appears to accelerate as estrogen drops.
- Frozen shoulder (adhesive capsulitis): heavily concentrated in women in their late 40s and 50s, and rare outside that window. The demographic overlap is not a coincidence.
- Connective-tissue stiffness and increased susceptibility to tendon problems (tendinopathy in the hip, shoulder, and Achilles).
The mechanistic thread through all of this is estrogen. Estrogen receptors sit in muscle satellite cells, in bone remodeling cells, in cartilage chondrocytes, in tendon, and in the neural tissue that modulates joint pain perception. Falling estrogen sets off a cascade: less muscle protein synthesis response to a given training stimulus, faster bone resorption relative to formation, more cartilage matrix degradation, and altered pain signaling. That is why the individual complaints are related. They share a driver.
How Common, and How Disabling?
The most cited prevalence numbers, per the Wright review:
- More than 70 percent of women experience musculoskeletal symptoms during the perimenopause-to-postmenopause transition.
- About 25 percent are functionally disabled by musculoskeletal symptoms at some point during the transition.
- Roughly 47 million women globally enter the transition each year.
- Arthralgia specifically affects over half of women in the perimenopausal window.
The disability piece is the part that gets under-reported. When we say 25 percent disabled, that means women who cannot climb stairs comfortably, cannot lift a grocery bag without wincing, cannot reach overhead, or cannot sleep on one side because a shoulder locks. These are not people who "just" have some joint pain. They are people whose baseline function has meaningfully dropped.
There is also a fibromyalgia signal in this population that reinforces the pattern. A 2024 review by Vidal-Neira et al. in Climacteric reports that fibromyalgia symptoms often begin during menopause and severity worsens after hysterectomy (with or without ovarian removal), consistent with a hormonal contribution. Earlier work by Blümel et al. (2012) in Maturitas argued from epidemiological, symptomatic, and therapeutic similarity that fibromyalgia may itself be part of the climacteric syndrome. Not everyone with menopausal musculoskeletal symptoms develops fibromyalgia, but the temporal clustering suggests a shared inflammatory or central pain-modulation mechanism.
Why Estrogen Matters for Muscle, Bone, and Joints
The mechanistic case in the Wright review pulls from several lines of evidence.
Muscle. Skeletal muscle expresses estrogen receptors, and estrogen appears to modulate satellite cell activity and myofibrillar protein synthesis. As estrogen falls, the anabolic response to a given amount of resistance training or dietary protein appears blunted. This is one reason women in the menopausal transition often notice that the same amount of activity produces less result than it used to. Not "less willpower". Less biological response.
Bone. Estrogen restrains osteoclast activity. When estrogen drops, osteoclast-driven resorption outpaces osteoblast-driven formation, and bone density declines. The steepest window is the perimenopausal transition and the first few post-menopausal years. This is well-established endocrinology and is not new to the Wright framing.
Cartilage and joints. Cartilage chondrocytes have estrogen receptors. Estrogen appears to reduce matrix metalloproteinase activity (the enzymes that break cartilage down) and modulate inflammatory cytokine release in the joint. Falling estrogen tips the balance toward degradation and inflammation, which shows up as arthralgia and, over years, accelerated osteoarthritis.
Central pain modulation. Estrogen is neuroactive. It appears to blunt central pain sensitization. Reduced estrogen may increase sensitivity to nociceptive signals, which contributes to the "everything hurts more" experience some women describe. This is also mechanistically consistent with the climacteric-fibromyalgia clustering.
Get an evidence-based plan built for you
FitCraft, our mobile fitness app, pairs you with an AI coach who builds you a personalized plan around your goals, schedule, and fitness level. Every FitCraft program is designed by Domenic Angelino, MPH (Brown University) and NSCA-CSCS, with research published in the Journal of Strength and Conditioning Research and Medicine & Science in Sports & Exercise.
Take the Free Assessment Free • 2 minutes • No credit cardThe Strongest Exercise Trial: LIFTMOR (Watson et al., 2018)
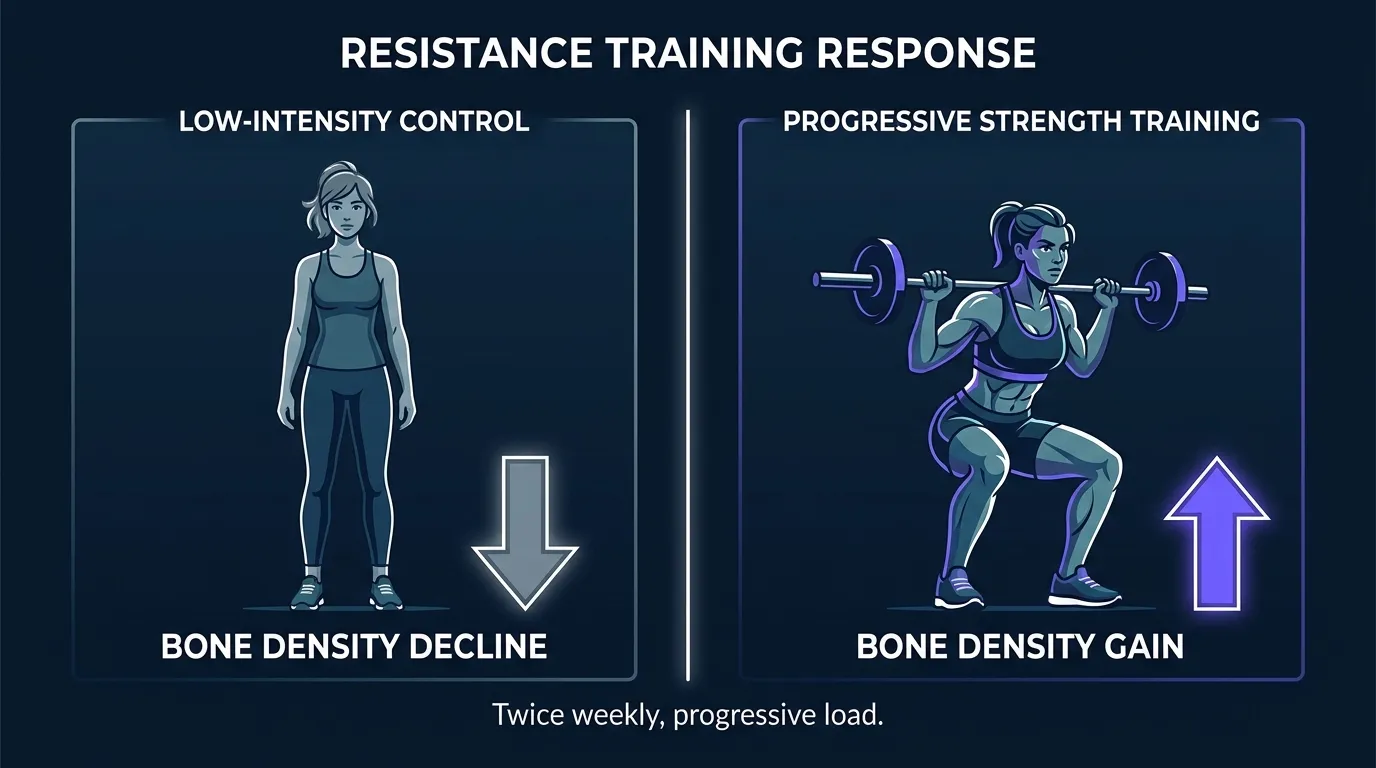
If you want to know what the highest-quality randomized data says about reversing pieces of this syndrome, the LIFTMOR trial is the reference. Watson, Weeks, Weis, Harding, Horan, and Beck (2018) in the Journal of Bone and Mineral Research randomized 101 postmenopausal women with low bone mass (T-score below -1.0) to one of two arms:
- Intervention: 8 months of twice-weekly, 30-minute supervised resistance and impact training. The resistance work was heavy (deadlifts, overhead press, back squats at more than 85 percent of one-rep max, 5 sets of 5 reps). The impact component was jumping chin-ups with drop landings.
- Control: a home-based, low-intensity exercise program.
What they found:
- Lumbar spine bone mineral density: +2.9 percent in the intervention group versus -1.2 percent in control (between-group difference 4.1 percent, p<0.001). Real bone gained, not just slowed loss.
- Femoral neck bone mineral density: +0.3 percent versus -1.9 percent (between-group difference 2.2 percent, p<0.05).
- Functional performance: significant improvements in the timed up-and-go, functional reach, back extensor strength, leg press strength, and 5-times sit-to-stand.
- Adherence and safety: average adherence above 90 percent. No serious adverse events. One participant with pre-existing spondylolysis was withdrawn.
The takeaway is not "everyone must deadlift 85 percent of their max." The takeaway is that the highest-quality trial data available shows postmenopausal bone loss is genuinely reversible with progressive, sufficiently loaded resistance training. Lighter loads produce smaller effects. Not zero, just smaller. Progressive loading with skilled programming matters more than any single exercise choice.
What About Estrogen Therapy for Joint Pain?
Menopausal hormone therapy (MHT, sometimes still called HRT) is a medical decision that belongs with your doctor. But there is randomized evidence on the joint-pain component specifically that is worth knowing.
In a post hoc analysis of the Women's Health Initiative (WHI) randomized trial, Chlebowski, Cirillo, Eaton, and colleagues (2013) in Menopause examined joint symptoms in the estrogen-alone arm. Ten thousand seven hundred thirty-nine postmenopausal women who had had a hysterectomy were randomized to conjugated equine estrogen or placebo. At 12 months:
- Joint pain frequency: 76.3 percent in the estrogen group versus 79.2 percent in placebo (p=0.001).
- Joint pain severity: modestly lower in the estrogen group, and the difference persisted through year 3.
- Joint swelling: modestly higher in the estrogen group (42.1 percent versus 39.7 percent, p=0.02). The pain effect and swelling effect ran in opposite directions.
The effect size on pain is not huge, but it is randomized, adequately powered, and consistent with the estrogen-receptor-in-cartilage mechanistic story. Estrogen alone does not eliminate joint pain, but it modestly reduces frequency and severity. The swelling finding running the other direction is worth flagging honestly, and Chlebowski et al. discussed it openly in the paper. That mixed picture matters for the roughly one-in-four women whose arthralgia is disabling.
Whether MHT is a right decision for a given woman is a conversation about individual risk-benefit balance: family history, cardiovascular risk, cancer risk, symptom severity, timing (starting within 10 years of the final menstrual period appears to be safer than starting much later). It is not a decision to make from an article. But the joint-pain component of the syndrome does have a specific evidence-based pharmacological option, and it is worth raising with your clinician if arthralgia is significantly affecting your life.
What Actually Helps: A Framework
Pulling the evidence together, here is what the research supports for someone in the perimenopausal or postmenopausal window who wants to work against the syndrome.
Progressive Resistance Training, Twice a Week Minimum
This is the intervention with the strongest evidence for reversing pieces of the syndrome. Watson et al. used high-intensity work, but progressive resistance training at any starting point matters more than absolute load. Start where you are, load enough to feel it, add weight or reps over time. Cover major compound movements: hinge, squat, push, pull, carry. Twice a week is the floor for bone effect. Three times a week is better for muscle. The pattern applies to perimenopause, post-menopause, and beyond.
Some Impact Work, Progressed Sensibly
Bone responds to impact plus resistance more than to either alone. Impact does not mean box jumps on day one. It can be heel drops, hopping in place, skipping, low-box step-downs. Progress from lower to higher based on how you feel and what your bone density starting point is. If you have osteoporosis (not just osteopenia), the impact progression needs medical clearance.
Enough Protein to Support Muscle Anabolism
The blunted anabolic response in this window means the "cover it with 60 grams a day" rule of thumb from earlier adulthood is often not enough. Most literature on older adults points toward 1.2 to 1.6 g/kg of body weight per day, spread across meals, with 30 to 40 grams per meal to hit the leucine threshold. This is a nutrition conversation. It supports the training but does not replace it.
Balance and Mobility, Because Falls Compound Everything
Fall-related fractures are one of the ways the syndrome does its worst damage. Balance work does not need to be complicated. Single-leg standing, tandem stance, and controlled step patterns integrated into normal training keep the balance system trained. We cover the underlying research in our balance training and falls writeup.
Sleep and Stress Management, Because Both Modulate Pain
Sleep quality drops in the menopausal transition (hot flashes, altered circadian rhythms), and poor sleep amplifies pain perception. Structured wind-down, cool sleep environment, consistent schedule. These are not glamorous interventions, but they compound with the training and nutrition side.
The Medical Conversation
For women with disabling arthralgia, significant bone loss, or severe symptoms, this is a medical picture. Menopausal hormone therapy, bisphosphonates, and other options exist. The 2024 Wright review's core message is not "do it yourself"; it is "recognize the syndrome and get it treated as a syndrome". That treatment is a mix of movement, nutrition, and where appropriate, medication.
What the Research Suggests Going Forward
The syndrome framing is new, but it consolidates evidence that has been accumulating for two decades. The practical implications are clear enough now.
First, do not treat menopausal joint pain, muscle loss, and bone loss as separate age-related complaints. They share a driver. Treating them together, with a coherent plan, is more effective than treating them piecemeal.
Second, resistance training is not optional for women in this window. The strength-training-after-60 evidence and the LIFTMOR data on postmenopausal women in their 60s and 70s both support this. The stimulus needs to progress. The volume needs to be regular. Twice a week is the floor.
Third, the medical conversation is worth having. Menopausal hormone therapy for symptom relief within the 10-year window is being reappraised in current guidelines, and joint symptoms are one component. Bisphosphonates and other bone-directed medications are the appropriate response for diagnosed osteoporosis. Neither is instead of movement. Both can complement it.
The bigger picture is a shift in how the healthcare system thinks about midlife women. For a long time the message was to expect decline. The research says decline is real, but a large chunk of it is reversible, and a coherent plan makes more difference than most people are told.
How FitCraft Fits
Most fitness apps default to programs designed for men in their 20s and 30s. The load progression, the volume, and the exercise selection are all pitched at a different biology.
FitCraft pairs you with an AI coach who builds your plan around the goals and constraints you share at signup. For a woman in her 40s or 50s coming into resistance training for the first time, the right starting point is not what shows up in a generic template. Progressive loading, appropriate exercise selection, and the ability to scale as you build capacity are what matter. That progression, structured over months, is what the research shows produces the bone and muscle response.
References
- Wright VJ, Schwartzman JD, Itinoche R, Wittstein J. "The musculoskeletal syndrome of menopause." Climacteric. 2024;27(5):466-472. doi:10.1080/13697137.2024.2380363 (PMID 39077777).
- Watson SL, Weeks BK, Weis LJ, Harding AT, Horan SA, Beck BR. "High-Intensity Resistance and Impact Training Improves Bone Mineral Density and Physical Function in Postmenopausal Women With Osteopenia and Osteoporosis: The LIFTMOR Randomized Controlled Trial." Journal of Bone and Mineral Research. 2018;33(2):211-220. doi:10.1002/jbmr.3284 (PMID 28975661).
- Chlebowski RT, Cirillo DJ, Eaton CB, et al. "Estrogen alone and joint symptoms in the Women's Health Initiative randomized trial." Menopause. 2013;20(6):600-608. doi:10.1097/GME.0b013e31828392c4 (PMID 23511705).
- Vidal-Neira LF, Neyro JL, Maldonado G, et al. "Climacteric and fibromyalgia: a review." Climacteric. 2024;27(5):458-465. doi:10.1080/13697137.2024.2376190 (PMID 39037037).
- Blümel JE, Palacios S, Legorreta D, Vallejo MS, Sarra S. "Is fibromyalgia part of the climacteric syndrome?" Maturitas. 2012;73(2):87-93. doi:10.1016/j.maturitas.2012.06.001 (PMID 22771264).
Frequently Asked Questions
What is the musculoskeletal syndrome of menopause?
It is the collective name for the cluster of musculoskeletal changes that show up as estrogen falls during the menopausal transition. The term was proposed in a 2024 Climacteric review by Wright, Schwartzman, Itinoche, and Wittstein. The core cluster: joint pain (arthralgia), loss of muscle mass and strength (sarcopenia), loss of bone mineral density, progression of osteoarthritis, frozen shoulder, and general soft-tissue stiffness. The Wright review reports that more than 70 percent of women experience musculoskeletal symptoms across the perimenopause-to-postmenopause transition, and about 25 percent are functionally disabled by them at some point during the transition.
Does resistance training help musculoskeletal symptoms of menopause?
Yes, and it is the single best-supported non-pharmacological intervention. The LIFTMOR randomized controlled trial by Watson et al. (2018) in the Journal of Bone and Mineral Research randomized 101 postmenopausal women with low bone mass to 8 months of twice-weekly supervised resistance and impact training or a home-based low-intensity control. The trained group gained 2.9 percent at the lumbar spine and 0.3 percent at the femoral neck, versus losses in the control group, with a between-group difference of 4.1 percent at the spine. Timed up-and-go, back extensor strength, and functional reach all improved significantly. Adherence was over 90 percent. Resistance training also directly addresses sarcopenia and helps arthralgia by loading joints in controlled ranges of motion.
How much does estrogen actually contribute to joint pain?
Enough that reintroducing it reduces reported joint pain. In a post hoc analysis of the Women's Health Initiative randomized trial by Chlebowski et al. (2013) in Menopause, women randomized to conjugated equine estrogen alone reported joint pain at 12 months at a rate of 76.3 percent, versus 79.2 percent in the placebo group. The absolute difference was small but statistically significant across 10,739 women. Joint swelling actually ran modestly higher in the estrogen arm (42.1 percent versus 39.7 percent, p=0.02), so the effect is on pain frequency and severity, not swelling. Estrogen receptors sit in cartilage, tendon, muscle, and bone tissue, and estrogen appears to modulate joint inflammation and connective-tissue turnover. This is one of the mechanistic pieces behind why the syndrome emerges as estrogen falls.
Is this the same as osteoporosis?
No. Osteoporosis is one component of the syndrome, not the whole thing. The musculoskeletal syndrome of menopause is broader: it also includes arthralgia (joint pain without an obvious mechanical cause), sarcopenia (muscle loss), osteoarthritis progression, frozen shoulder, and connective-tissue stiffness. The point of naming it as a syndrome, per Wright et al. (2024), is that the individual pieces are often treated as unrelated aging complaints. Recognizing them as a cluster driven by estrogen decline reframes the treatment approach toward resistance training, bone-loading exercise, and (where appropriate) menopausal hormone therapy under medical supervision.
Do I need heavy weights to protect my bones?
Higher loads produce stronger bone response, but not everyone starts there and progression matters more than absolute load. LIFTMOR trained women at more than 85 percent of one-rep max, which is heavy, and it worked. But dumbbell resistance training, resistance-band training, bodyweight strength work, and impact exercises like heel drops all produce measurable bone-loading stimulus, especially when built up progressively over months. The evidence-based rule is more about intensity relative to your current capacity than absolute weight. Twice-weekly progressive resistance training is the floor. Working with a coach who structures the progression matters, especially if you are new to lifting or have osteopenia.