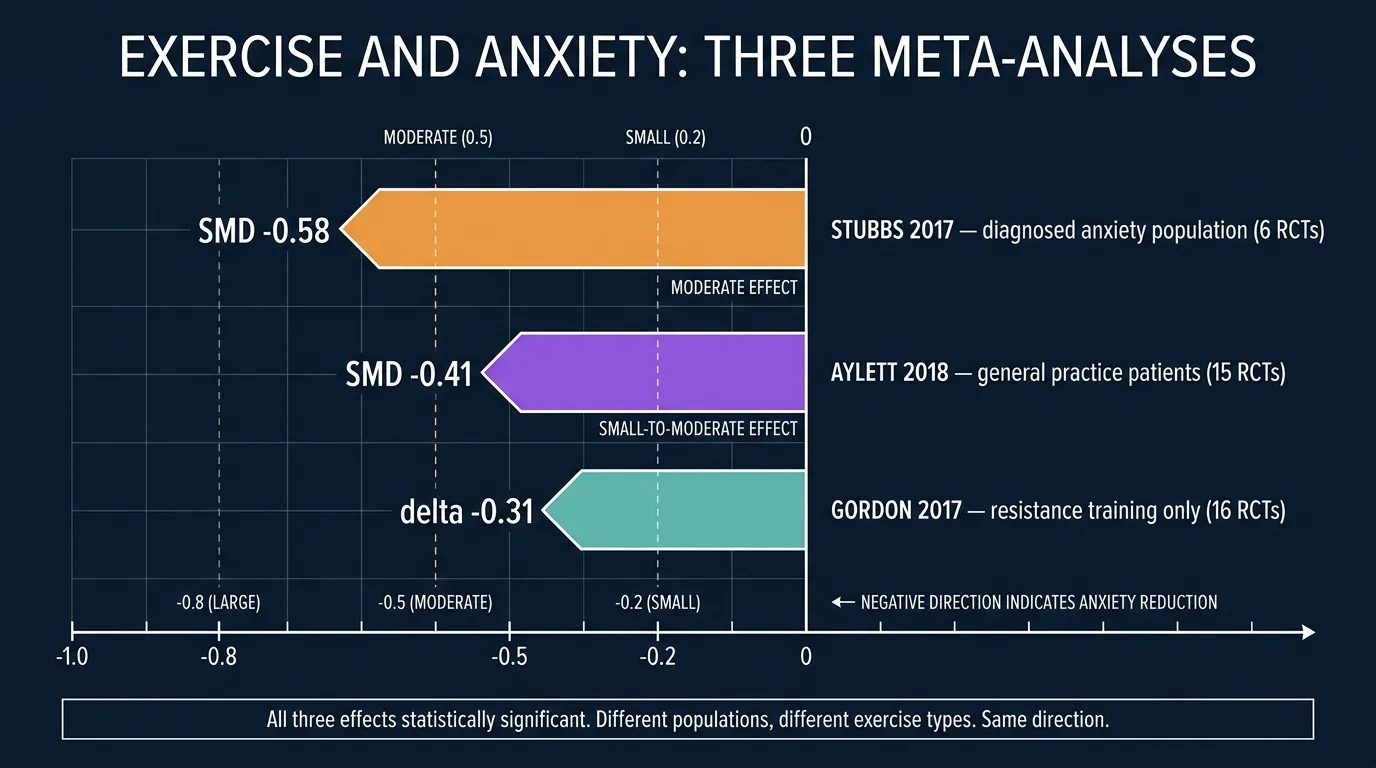
Here's the number to hold onto: -0.58.
That's the standardized mean difference, the effect size, that Brendon Stubbs and his co-authors calculated in 2017 after pooling six randomized controlled trials of adults with diagnosed anxiety or stress-related disorders. An effect around 0.5 is what clinicians call "moderate." It's the range where doctors start considering something a legitimate treatment tool. Not a miracle. Not a placebo. A real intervention with real signal.
And the wild part? This wasn't a single hopeful study. It's the pooled result of six of them. Which means when we ask "does exercise actually help anxiety, or is that just wishful thinking?" we can now answer with some numbers behind us.
The short answer: it does. But the honest, useful answer needs more context than a headline. So let's walk through what the research actually shows. What kind of exercise. How much. For whom. And where the limits are, because there are limits, and pretending otherwise is how we end up with people going off their meds after reading a blog post.
The Research: What the Major Studies Found
Stubbs et al. (2017): Exercise in People With Diagnosed Anxiety
The Stubbs meta-analysis matters because of who was in the trials. Not "college students who felt a bit stressed." Adults with a current clinical diagnosis of an anxiety disorder or a stress-related disorder (things like generalized anxiety disorder, panic disorder, and PTSD).
The team pooled six RCTs comprising 262 participants and compared aerobic and resistance exercise to control conditions. The result:
- 6 randomized controlled trials in adults with diagnosed anxiety or stress-related disorders
- SMD of -0.582 favoring exercise (p = 0.02)
- Both aerobic and resistance modalities were represented in the pool
- The authors concluded exercise should be considered an important treatment option alongside standard care
An effect size around 0.5 is what psychologists call a moderate effect. For context, that's in the same neighborhood as psychotherapy for anxiety in some head-to-head comparisons. It's smaller than the exercise effect Schuch found for depression (SMD -1.11), which lines up with the broader research: exercise consistently helps anxiety, but the effect is a bit more modest than what shows up for depression.
Citation: Stubbs B, Vancampfort D, Rosenbaum S, et al. An examination of the anxiolytic effects of exercise for people with anxiety and stress-related disorders: A meta-analysis. Psychiatry Res. 2017;249:102-108.
Aylett et al. (2018): Anxiety in General Practice
Not everyone with anxiety symptoms has a formal diagnosis. A lot of anxiety shows up in the GP's office as "I can't sleep," "my chest feels tight," "I'm on edge all the time." Elizabeth Aylett and colleagues went looking for what happens when general practice doctors prescribe exercise for these patients.
Their 2018 systematic review in BMC Health Services Research pooled 15 randomized controlled trials involving 675 patients. Aerobic exercise vs. waiting-list controls. The findings:
- 15 randomized controlled trials conducted in general practice or primary care settings
- 675 total patients with anxiety symptoms
- SMD of -0.41 (95% CI -0.70 to -0.12) comparing aerobic exercise to waiting list
- High-intensity regimens outperformed low-intensity regimens, a dose-response signal
An effect around 0.4 is smaller than what Stubbs found in the clinical anxiety population, but it's still meaningful. And it's more generalizable to the "walking wounded" of everyday anxiety. The people who wouldn't necessarily meet DSM criteria but who are absolutely suffering.
Aylett's finding that intensity matters is worth pausing on. It's a common misconception that mental-health exercise has to be gentle. The research keeps pointing the other direction. Vigorous work does more.
Citation: Aylett E, Small N, Bower P. Exercise in the treatment of clinical anxiety in general practice: a systematic review and meta-analysis. BMC Health Serv Res. 2018;18(1):559.
Gordon et al. (2017): Resistance Training, Specifically
Most anxiety research has focused on aerobic exercise. So Brett Gordon and colleagues went and looked at resistance training on its own. Their 2017 meta-analysis in Sports Medicine pooled 16 RCTs (31 effects) totaling 922 participants.
The result: resistance training significantly reduced anxiety symptoms (Δ = 0.31, 95% CI 0.17 to 0.44, p < 0.001).
That's a small-to-moderate effect. Notably, the anxiety reductions were larger among healthy participants than among those with an existing physical or mental illness, which is an interesting inversion of what we see in depression research. Reading between the lines: resistance training may be especially useful as a preventive tool, catching low-grade anxiety before it becomes clinical.
The Gordon paper also demolished a common myth. You don't need to lift heavy to get the anxiety benefit. Effect sizes were consistent across programs using bodyweight, light-load, and moderate-load protocols. Which is convenient, because most people aren't going to squat 300 pounds to feel calmer.
Citation: Gordon BR, McDowell CP, Lyons M, Herring MP. The Effects of Resistance Exercise Training on Anxiety: A Meta-Analysis and Meta-Regression Analysis of Randomized Controlled Trials. Sports Med. 2017;47(12):2521-2532.
Herring et al. (2010): Anxiety in People With Chronic Illness
What happens when you layer anxiety on top of something else, cancer, heart disease, chronic pain? Matthew Herring and colleagues at the University of Georgia asked that in 2010 in the Archives of Internal Medicine. They pooled 40 trials with 2,914 sedentary adults living with chronic illness.
The takeaway: exercise reduced anxiety symptoms across the board, by roughly 20% on average versus control conditions. The effect held across cancer patients, cardiac patients, patients with chronic pain, and patients with multiple sclerosis. It also held when researchers restricted analysis to studies with intent-to-treat designs (a stricter test).
Why this matters: anxiety is often collateral damage of chronic disease. This is the meta-analysis that gave clinicians permission to prescribe exercise as part of comprehensive care, not just for the physical benefits but for the mental ones too.
Citation: Herring MP, O'Connor PJ, Dishman RK. The effect of exercise training on anxiety symptoms among patients: a systematic review. Arch Intern Med. 2010;170(4):321-331.
Singh et al. (2023): The Umbrella Review
Zoom out further. In 2023, Ben Singh and colleagues published an umbrella review, a review of reviews, in the British Journal of Sports Medicine. It synthesized 97 systematic reviews covering 1,039 trials and 128,119 participants.
Their conclusion was direct: physical activity is highly effective for reducing symptoms of depression, anxiety, and distress across a wide range of populations, and effects were larger with vigorous intensity compared to light or moderate activity. That's not one study anymore. That's more than a thousand trials pointing the same way.
Citation: Singh B, Olds T, Curtis R, et al. Effectiveness of physical activity interventions for improving depression, anxiety and distress: an overview of systematic reviews. Br J Sports Med. 2023;57(18):1203-1209.
Why This Matters if You've Been Struggling
If you're reading this because anxiety has been running your life, the racing thoughts, the tight chest, the 3 a.m. review of every awkward thing you've ever said, you're not broken and you're not alone. Anxiety disorders are the most common mental health condition worldwide, affecting an estimated 301 million people in 2019 according to the World Health Organization.
Look, telling someone in the middle of an anxiety spiral to "just go for a run" is not helpful. In some cases it's actively wrong, exercise can briefly increase heart rate and breathing in ways that mimic the physical sensations of anxiety, which some people find distressing before they find it grounding. That's a real thing. It's called anxiety sensitivity, and we'll come back to it.
What the research offers isn't a lecture. It's evidence. If you can find a way to move your body regularly, even imperfectly, the benefits are measurable and comparable to other well-established anxiety treatments. And once you get past the first few weeks (which are the hard part), the effect tends to grow.
How Exercise Actually Reduces Anxiety: The Mechanisms
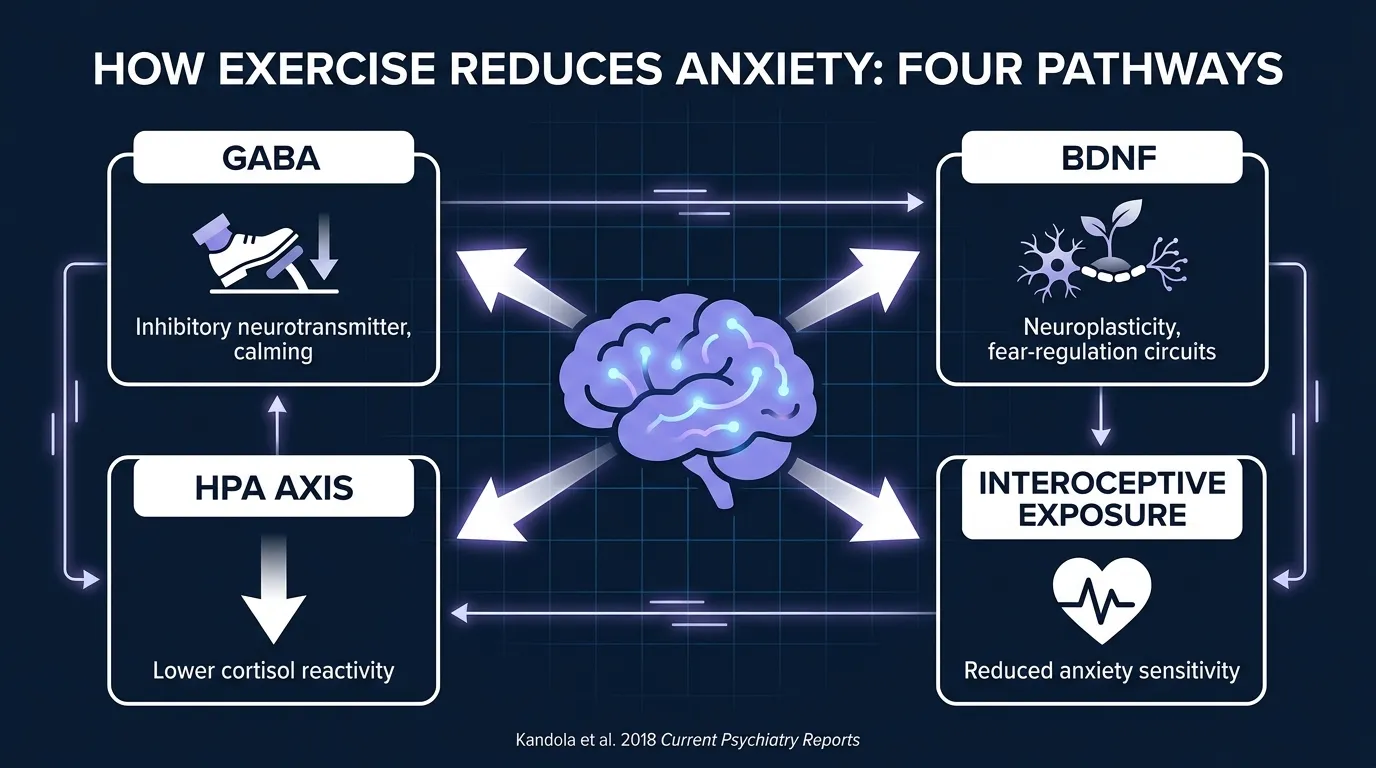
Kandola and colleagues 2018 in Current Psychiatry Reports reviewed the therapeutic and epidemiological picture around physical activity and anxiety, and flagged several plausible mechanisms. Combined with the broader neuroscience literature, four pathways get the most attention. Here's the practical version.
GABA: Your Brain's Brake Pedal
GABA (gamma-aminobutyric acid) is the main inhibitory neurotransmitter in your brain. It's what benzodiazepines like Xanax and Ativan boost. It's what alcohol partially mimics. Low GABA is one of the more consistent findings in anxiety disorders.
Aerobic exercise, in particular, increases GABA levels and improves GABA receptor sensitivity. Human MRS imaging studies have documented measurable GABA increases in cortical regions after single exercise bouts. So the "calm" you feel after a hard workout? Not just endorphins. There's actual chemistry there, using overlapping pathways to the drugs prescribed for the same problem.
BDNF and Neuroplasticity
Brain-derived neurotrophic factor. The same protein that shows up in the depression research. Anxiety disorders are associated with reduced BDNF and hippocampal atrophy. Exercise boosts BDNF, promotes neurogenesis, and appears to help the brain regions responsible for regulating fear responses (particularly the prefrontal cortex to amygdala circuit) function more effectively.
Translation: exercise physically helps the parts of your brain that are supposed to say "wait, this isn't actually dangerous" do their job.
HPA Axis Downregulation
The hypothalamic-pituitary-adrenal axis controls your body's stress response. In chronic anxiety, this system tends to be dysregulated. Baseline cortisol is elevated, reactivity to stressors is exaggerated, recovery from stress is delayed.
Regular exercise appears to recalibrate the HPA axis. Trained individuals show blunted cortisol responses to psychological stressors and faster recovery. It's like slowly detuning a smoke alarm that's been going off too easily.
Interoceptive Exposure (Yes, This Is a Real Thing)
This one is fascinating. Anxiety sensitivity, the fear of the physical sensations of anxiety itself, is a huge driver of panic disorders. Elevated heart rate, sweating, shortness of breath, dizziness. These sensations become inherently frightening because they're linked to panic.
Exercise creates the same sensations, but in a safe context. Repeated exposure to a racing heart during a run, without any actual danger, gradually decouples the sensations from the fear response. It's a form of exposure therapy your body does on you, without you having to schedule it. Wait, that sounds ominous, let me put it differently. Exercise gives your body regular practice at feeling activated without spiraling. Over weeks and months, that practice starts to translate into calmer responses in real anxiety-provoking situations.
Enjoying the article?
Start a new fitness routine today, written by me and coached by the AI I designed.
Take the Free Assessment Free • 2 minutes • No credit cardHow Much? What Type? A Practical Read of the Data
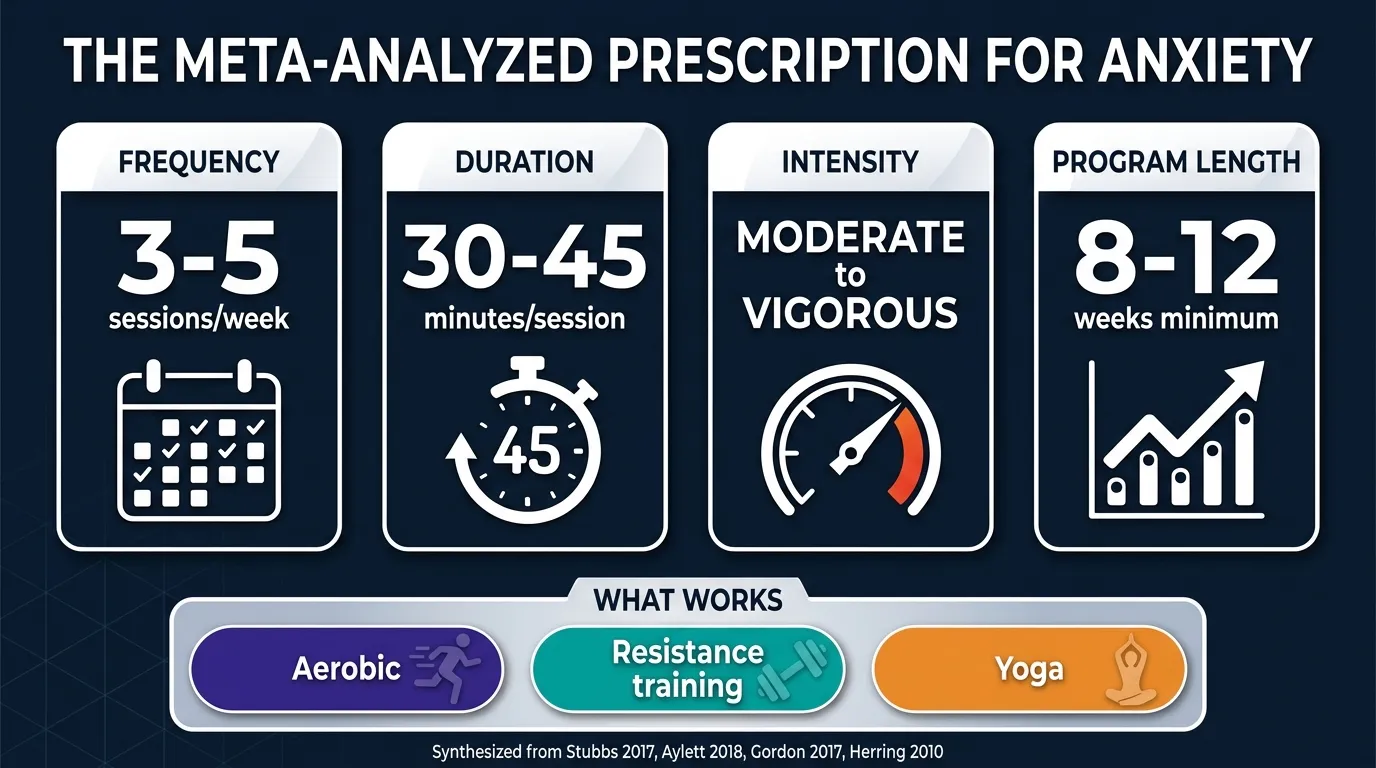
Here's the summary a clinician would give you, based on what pools out of the meta-analyses.
Frequency: 3 to 5 sessions per week. Below 3 you're under-dosed. Above 5 you're not necessarily getting more benefit and you may risk burnout.
Duration: 30 to 45 minutes per session for the meta-analyzed effect sizes. Shorter bouts (10 to 20 minutes) still produce acute anxiety reduction, but the training effect on baseline anxiety seems to require some minimum time under load.
Intensity: Moderate to vigorous. Aylett's meta-analysis explicitly found high-intensity regimens beat low-intensity ones. Kandola's review reached the same conclusion. That doesn't mean sprinting. It means a heart rate where you can talk but not sing.
Duration of program: Most trials showing solid effects ran 8 to 12 weeks. That's the "give it a real shot" window. Two weeks of good workouts followed by quitting isn't going to move the needle much.
Modality: Aerobic has the largest evidence base. Resistance training works too (Gordon 2017). Yoga also shows benefits, particularly for generalized anxiety. Some limited but promising evidence for tai chi. Pick whichever you'll do consistently for 3 months.
Common Misconceptions
Misconception: "Exercise makes my anxiety worse because I feel my heart pounding"
Reality: partially true, and it can flip. If you have high anxiety sensitivity or panic disorder, the physical sensations of exercise can absolutely feel activating in the short term. That's real and it's not your imagination. The counterintuitive move is to work with it, not against it. Repeated exposure, ideally with therapist support if you have panic disorder, is exactly how CBT protocols like interoceptive exposure therapy work. Start with lower intensity, build up gradually, and let your nervous system learn that the sensations aren't dangerous.
Misconception: "You need intense cardio for the anxiety benefit"
Reality: intensity helps, but it's not the whole story. Yes, higher-intensity work tends to produce larger anxiety reductions. But that dose-response curve isn't infinite. Resistance training at moderate loads works (Gordon 2017). Yoga works. Even walking has evidence, especially for acute anxiety reduction after a single session. The biggest jump is between "nothing" and "something." The jump between "something" and "a lot" is smaller.
Misconception: "If exercise hasn't helped my anxiety, I'm doing it wrong"
Reality: anxiety is heterogeneous. The umbrella term "anxiety" covers generalized anxiety disorder, panic disorder, social anxiety, specific phobias, PTSD, and health anxiety. Different mechanisms, different responses. If you've been exercising consistently for 8 to 12 weeks and haven't seen improvement, that's useful information for a clinician, not evidence of personal failure. Some people need therapy. Some need medication. Most benefit from combining tools.
Misconception: "Exercise can replace my anxiety medication"
Reality: no. This is the most dangerous misreading, and we want to be direct. The meta-analyses show exercise has anxiolytic effects. They do not show exercise as a standalone replacement for medication, especially in moderate-to-severe anxiety disorders. If you're on medication for anxiety, do not stop or reduce it based on an exercise routine alone. Talk to your prescriber. Exercise almost always works better alongside standard care than instead of it.
The Consistency Problem (And Why It's Worse for Anxiety)
Here's the awkward truth. Exercise only works if you keep doing it. And anxiety, specifically, makes that harder than depression does.
Why? Because anxiety often produces avoidance. Gym anxiety. Social anxiety about being seen exercising. Perfectionism that says "if I can't do the full 45 minutes, why bother." Panic sensitivity that makes elevated heart rate feel scary. The very condition you're trying to treat is actively resisting the treatment.
That's not a personal failing. It's the disorder doing what disorders do. The fix isn't more willpower (see our piece on the willpower myth). It's designing an approach that works around anxiety's specific patterns.
A few things that help:
- Home workouts remove the social and environmental triggers. There's a reason our gym anxiety guide exists.
- Predictable structure. Anxiety hates uncertainty. Following a program removes the "what should I do today?" decision that becomes a trigger for procrastination.
- Small, non-negotiable minimums. "I will do 10 minutes today" beats "I will do 45 minutes today" because the 10-minute promise is one you can keep on your worst days.
- Tracking that shows momentum. Streaks, XP, or even a paper habit tracker helps counter anxiety's tendency to erase the memory of your wins.
Research on gamification and exercise adherence shows that programs using progress mechanics produce higher long-term adherence than programs relying on motivation alone. For someone with anxiety, "not depending on motivation" is exactly the point.
Where the Evidence Ends
To be fair to the science, let me flag what we don't yet have solid answers on.
Optimal dose. The 30 to 45 minutes, 3 to 5 times a week range is a synthesis of what most trials used, not proof it's ideal. It's plausible that shorter, more frequent sessions could be equivalent. The research isn't fine-grained enough to say yet.
Long-term maintenance. Most trials ran 8 to 24 weeks. The multi-year picture is thinner. What happens if you exercise consistently for two years and then stop? Do gains hold? Fade? Depend on the person? We don't have great data.
Anxiety subtype-specific effects. Some evidence suggests exercise is particularly helpful for panic disorder and generalized anxiety, and less clear for OCD or specific phobias. But most trials lump anxiety types together, which makes subtype-specific claims hard to defend.
Interaction with medication and therapy. A few trials have looked at exercise as an add-on to SSRIs or CBT, and the early signal is that combinations work better than either alone. But the field needs more of these.
Here's the honest summary: the "does exercise help anxiety" question is settled. The "how, for whom, in what doses, combined with what" questions are still being worked out. Which is normal for a maturing area of research.
What This Means for You
Look, if you take one thing from this article, take this: exercise is one of the most consistently supported non-pharmacological tools for anxiety. It's not a magic bullet. It won't replace therapy or medication when those are needed. But if you can build a habit around it, the evidence base is genuinely strong.
The catch is the same catch that shows up in every mental health intervention. The tool only works if you use it. Repeatedly. Over weeks and months. Which for someone with anxiety is precisely the hard part.
We're not going to pretend FitCraft treats anxiety. It doesn't. It's a fitness app, not a medical device. What FitCraft does is help you solve the consistency problem, which, as this whole article makes clear, is the actual bottleneck.
Ty, the 3D AI personal trainer in the free version, adapts workouts to your level, equipment, and goals. Programming spans yoga, strength, cardio, and mobility. The gamification (XP, levels, streaks, collectible rewards) is designed to keep you engaged when motivation dips. And motivation will dip. That's biology. That's the disorder. Building a system that doesn't depend on motivation is the whole strategy.
Programs are designed by Domenic Angelino, an Ivy League-trained exercise scientist (MPH, Brown University; NSCA-CSCS) who built the AI coaching engine behind Ty. Every design decision maps to peer-reviewed findings, including the ones cited in this article. Research on fitness apps and mental health shows that the right design lowers the psychological barrier to getting started, which is often the biggest hurdle for people with anxiety.
If you want to try building a consistent exercise habit, and you want something that adapts to you rather than demanding you adapt to it, the free assessment takes two minutes.
References
- Stubbs B, Vancampfort D, Rosenbaum S, Firth J, Cosco T, Veronese N, Salum GA, Schuch FB. "An examination of the anxiolytic effects of exercise for people with anxiety and stress-related disorders: A meta-analysis." Psychiatry Research 249 (2017): 102-108. doi:10.1016/j.psychres.2016.12.020
- Aylett E, Small N, Bower P. "Exercise in the treatment of clinical anxiety in general practice: a systematic review and meta-analysis." BMC Health Services Research 18.1 (2018): 559. doi:10.1186/s12913-018-3313-5
- Gordon BR, McDowell CP, Lyons M, Herring MP. "The Effects of Resistance Exercise Training on Anxiety: A Meta-Analysis and Meta-Regression Analysis of Randomized Controlled Trials." Sports Medicine 47.12 (2017): 2521-2532. doi:10.1007/s40279-017-0769-0
- Herring MP, O'Connor PJ, Dishman RK. "The effect of exercise training on anxiety symptoms among patients: a systematic review." Archives of Internal Medicine 170.4 (2010): 321-331. doi:10.1001/archinternmed.2009.530
- Kandola A, Vancampfort D, Herring M, Rebar A, Hallgren M, Firth J, Stubbs B. "Moving to Beat Anxiety: Epidemiology and Therapeutic Issues with Physical Activity for Anxiety." Current Psychiatry Reports 20.8 (2018): 63. doi:10.1007/s11920-018-0923-x
- Singh B, Olds T, Curtis R, et al. "Effectiveness of physical activity interventions for improving depression, anxiety and distress: an overview of systematic reviews." British Journal of Sports Medicine 57.18 (2023): 1203-1209. doi:10.1136/bjsports-2022-106195
Frequently Asked Questions
Does exercise really help anxiety?
Yes. The Stubbs et al. (2017) meta-analysis of six RCTs in people with diagnosed anxiety and stress-related disorders found a moderate anxiolytic effect (SMD -0.58). The Aylett et al. (2018) BMC review of 15 trials in general practice found a smaller but significant effect (SMD -0.41), with higher-intensity exercise outperforming lower-intensity regimens. Effects are consistent across aerobic exercise, resistance training, and yoga.
What type of exercise is best for anxiety?
The research supports several options. Aerobic exercise has the largest evidence base for anxiety, with meta-analyses showing moderate effect sizes. Resistance training also reduces anxiety symptoms (Gordon et al. 2017 found Δ=0.31 across 16 RCTs). Yoga combines movement with breath control and shows benefits especially for generalized anxiety. The best exercise for your anxiety is the one you'll do consistently for at least 8 to 12 weeks.
How much exercise do you need to reduce anxiety?
Meta-analytic evidence suggests 30 to 45 minutes of moderate-to-vigorous exercise 3 to 5 days per week produces measurable anxiety reductions after 8 to 12 weeks. The Aylett meta-analysis specifically noted that high-intensity regimens outperformed low-intensity ones. That said, even short bouts of walking can produce acute anxiety reduction lasting several hours, so partial doses still count.
How does exercise reduce anxiety biologically?
Exercise triggers several parallel changes. It increases GABA, the brain's main inhibitory neurotransmitter (low GABA is linked to anxiety disorders). It boosts brain-derived neurotrophic factor (BDNF) and endocannabinoid signaling. Regular training also downregulates the HPA axis, reducing baseline cortisol reactivity. And repeated exposure to the physical sensations of exercise (elevated heart rate, breathing) can reduce anxiety sensitivity through a form of interoceptive exposure.
Can exercise replace medication or therapy for anxiety?
No. Exercise is a powerful adjunct, not a replacement for professional treatment, especially for diagnosed anxiety disorders. Meta-analyses consistently frame exercise as complementary to standard care. If you're on medication for anxiety, do not stop or reduce it based on an exercise routine alone. Talk to your prescriber. Exercise works best alongside therapy and, when indicated, medication.