
Here's a number that might surprise you: -1.11.
That's the standardized mean difference, the effect size, of exercise on depression, according to a landmark meta-analysis published in the Journal of Psychiatric Research in 2016. In clinical research, anything above 0.8 is considered a "large" effect. Exercise didn't just clear that bar. It vaulted over it.
The study, led by Felipe Schuch and colleagues, pooled data from 25 randomized controlled trials comparing exercise to control conditions in people with depression. After adjusting for publication bias, a correction that typically reduces effect sizes, exercise still showed a large, significant antidepressant effect. The fail-safe number was 1,057, meaning you'd need over a thousand null studies to erase the finding.
That's not a wellness blog opinion. That's a statistical wall.
But here's where it gets complicated, and where responsible science communication matters. Because "exercise helps depression" and "exercise replaces your medication" are very different statements. Only one of them is supported by the evidence. Let's break down what the research actually shows.
The Research: What the Major Studies Found
Schuch et al. (2016): The Landmark Meta-Analysis
The Schuch meta-analysis stands out for one critical reason: it adjusted for publication bias. That matters because studies showing positive results are more likely to get published than studies showing nothing. When you don't account for that, you get inflated numbers. Schuch's team used Duval and Tweedie's trim-and-fill procedure to correct for this, and exercise still showed a large effect.
Key numbers from the study:
- 25 randomized controlled trials comparing exercise to control groups
- SMD of -1.11 (95% CI: 0.79-1.43) after publication bias adjustment
- 9 trials specifically examined people with major depressive disorder (MDD), and the effect was even larger in this subgroup
- Larger effects were found for aerobic exercise, moderate-to-vigorous intensity, and both supervised and unsupervised formats
- Fail-safe number: 1,057, extremely robust against future null findings
To put that effect size in context: a meta-analysis of antidepressant medications typically shows an SMD around 0.30-0.50 compared to placebo. Exercise's -1.11 is larger. That doesn't mean exercise is "better" than medication. The comparisons aren't head-to-head, and there are important methodological differences. But it does mean the antidepressant effect of exercise is not small, not marginal, and not a placebo.
Citation: Schuch FB, Vancampfort D, Richards J, Rosenbaum S, Ward PB, Stubbs B. Exercise as a treatment for depression: A meta-analysis adjusting for publication bias. J Psychiatr Res. 2016;77:42-51.
Noetel et al. (2024): The Largest Analysis to Date
Eight years after Schuch, an even bigger study landed. Published in the BMJ in February 2024, Noetel and colleagues conducted a network meta-analysis, a technique that lets you compare multiple treatments against each other simultaneously, across 218 unique studies involving 14,170 participants.
This wasn't just "does exercise help?" It was "which type of exercise helps most, and how does it compare to medication and therapy?"
The results, compared to active controls:
- Walking or jogging: Hedges' g -0.62 (1,210 participants)
- Yoga: g -0.55 (1,047 participants)
- Strength training: g -0.49 (643 participants)
- Mixed aerobic exercise: g -0.43 (1,286 participants)
- Tai chi or qigong: g -0.42 (343 participants)
Two findings stand out. First, the antidepressant effect was proportional to intensity. Vigorous exercise produced stronger effects than light activity. Second, strength training and yoga had the highest adherence rates, which matters enormously. The most effective exercise for depression is the one you'll actually keep doing.
Citation: Noetel M, Sanders T, Gallardo-Gómez D, et al. Effect of exercise for depression: systematic review and network meta-analysis of randomised controlled trials. BMJ. 2024;384:e075847.
Singh et al. (2023): The Umbrella Review
If individual meta-analyses are convincing, what about a review of reviews? Singh and colleagues published exactly that in the British Journal of Sports Medicine in 2023. It was an umbrella review synthesizing 97 systematic reviews encompassing 1,039 trials and 128,119 participants.
Their conclusion was straightforward: physical activity is highly effective for improving symptoms of depression, anxiety, and psychological distress across a wide range of populations, including the general population, people with diagnosed mental health disorders, and people with chronic disease. Effects were stronger with vigorous intensity exercise compared to light and moderate activity.
That's not one study. That's a thousand trials. The signal is consistent.
Citation: Singh B, Olds T, Curtis R, et al. Effectiveness of physical activity interventions for improving depression, anxiety and distress: an overview of systematic reviews. Br J Sports Med. 2023;57(18):1203-1209.
It's Not Just Adults: Exercise and Youth Mental Health
Biddle and Asare's 2011 review of reviews in the British Journal of Sports Medicine examined physical activity and mental health specifically in children and adolescents (ages 5-17). They found small-to-moderate associations between physical activity and reduced depression, reduced anxiety, and improved self-esteem. The evidence also showed physical activity improved cognitive performance and classroom behavior, though these effects were smaller and less consistent.
By 2019, the number of systematic reviews on youth exercise and depression had quadrupled compared to when Biddle and Asare first counted them. The research base keeps growing, and the direction stays the same.
Citation: Biddle SJH, Asare M. Physical activity and mental health in children and adolescents: A review of reviews. Br J Sports Med. 2011;45(11):886-895.
Why This Matters for Your Mental Health
If you're reading this and you've been struggling, with low motivation, persistent sadness, that heavy fog that makes even small tasks feel enormous , you're not alone. Depression affects over 280 million people worldwide, according to the WHO. And the gap between knowing you should exercise and actually doing it can feel impossibly wide when you're in it.
That's not a willpower failure. It's the disease. Depression literally reduces the brain's capacity for motivation and reward processing. This is connected to what the research calls the willpower myth — the evidence is clear that relying on discipline alone doesn't work for most people. Telling someone with depression to "just go for a run" is like telling someone with a broken leg to walk it off. The intent might be good, but it ignores the reality.
What this research offers isn't a guilt trip about not exercising. It's hope , backed by data , that if you can find a way to move your body, even a little, even imperfectly, the benefits are real and measurable. And the research says the biggest barrier isn't finding the "right" exercise. It's finding one you'll do more than twice.
How Exercise Changes Your Brain: The Mechanisms
Exercise doesn't just "make you feel better" in some vague, hand-wavy way. It triggers specific neurobiological changes that directly counteract the brain changes associated with depression. Here's what's happening under the hood.
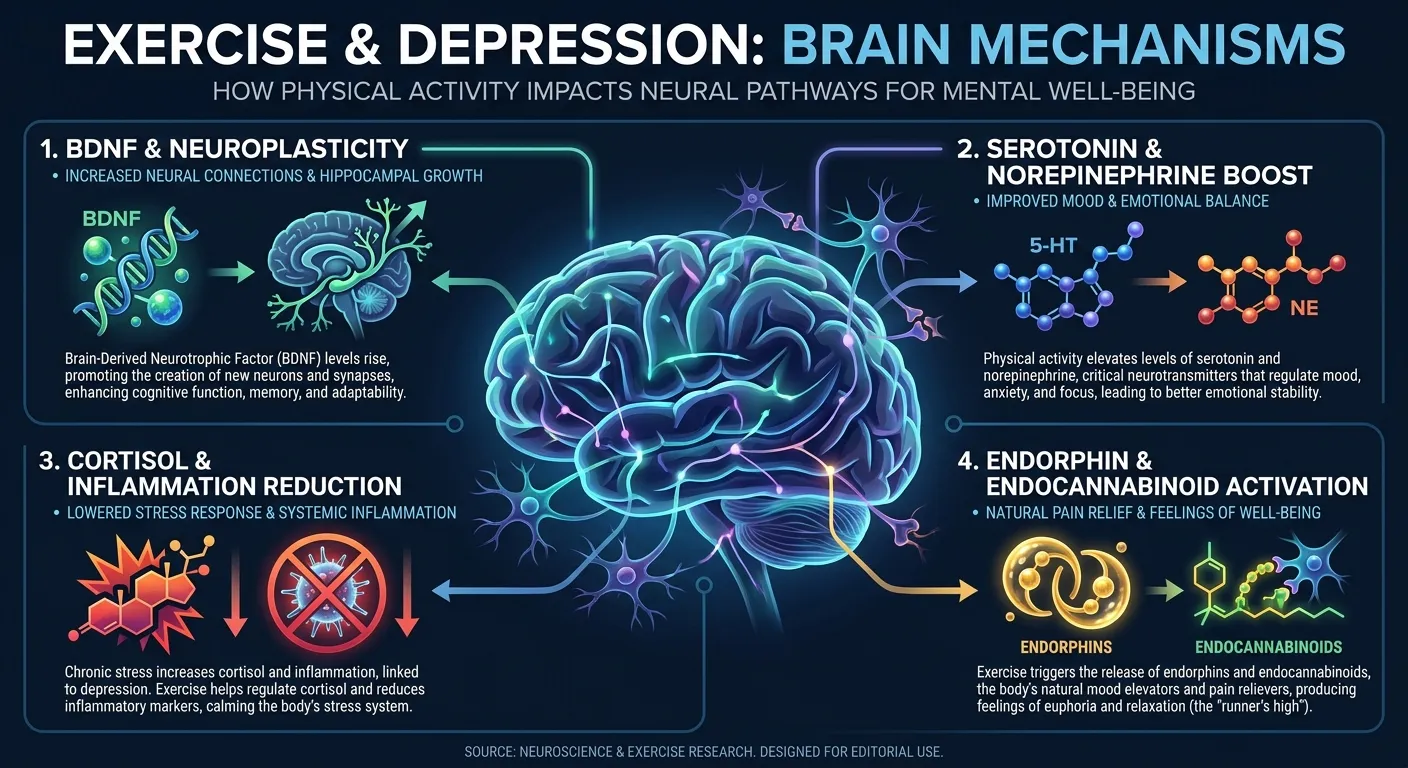
BDNF: Your Brain's Growth Factor
Brain-derived neurotrophic factor (BDNF) is a protein that promotes the survival, growth, and maintenance of neurons. Think of it as fertilizer for your brain. In people with depression, BDNF levels are consistently lower, and the hippocampus, a brain region critical for mood regulation and memory, actually shrinks during chronic depression.
Exercise increases BDNF levels. A 2017 review in Neural Plasticity by Phillips documented how physical activity promotes neuroplasticity, meaning the brain's ability to form new connections and grow new neurons, particularly in the hippocampus. This isn't subtle. Regular exercise can measurably increase hippocampal volume, partially reversing the structural brain changes caused by depression (Phillips, 2017).
Serotonin and Norepinephrine
Most antidepressant medications work by increasing the availability of serotonin, norepinephrine, or both. Exercise does the same thing, through a different mechanism, but with a similar downstream effect. Acute exercise bouts elevate both neurotransmitters, and regular training appears to improve the sensitivity of the receptors they bind to.
This biological overlap helps explain why exercise effect sizes are comparable to medication effect sizes. They're modifying overlapping pathways.
Cortisol and Inflammation
Depression is associated with elevated cortisol (the stress hormone) and chronic low-grade inflammation. Exercise reduces both. Regular physical activity lowers resting cortisol levels and decreases inflammatory markers like C-reactive protein and interleukin-6. Since inflammation itself can drive depressive symptoms. A growing area of research called the "inflammatory hypothesis of depression" , reducing it through exercise addresses a root mechanism, not just a symptom.
Endorphins (Yes, They're Real)
The "runner's high" isn't a myth, though it's more complex than the old endorphin story. Current research suggests the endocannabinoid system, the same system that cannabis activates, plays a significant role in the mood boost from exercise. But endorphins matter too, particularly for pain modulation and the sense of well-being that follows a hard workout.
Enjoying the article?
Start a new fitness routine today, written by me and coached by the AI I designed.
Take the Free Assessment Free • 2 minutes • No credit cardWhat the WHO Now Recommends
The World Health Organization's 2020 guidelines on physical activity explicitly recognize mental health benefits. Their recommendations:
- Adults: 150-300 minutes of moderate-intensity aerobic activity per week, or 75-150 minutes of vigorous-intensity activity
- Children and adolescents: At least 60 minutes per day of moderate-to-vigorous activity
- Mental health outcomes: Adults meeting these guidelines show reduced risk of depression (adjusted odds ratio 0.78) and anxiety (AOR 0.81) compared to inactive individuals
That 22% reduction in depression risk isn't trivial. At a population level, it would prevent millions of cases. At a personal level, it means the deck is meaningfully stacked in your favor if you can build a consistent habit.
The word "consistent" is doing heavy lifting in that sentence. And that's where most people get stuck.
Common Misconceptions
Misconception: "Exercise can replace my medication"
Reality: No. This is the most dangerous misreading of this research, and we want to be direct about it. The meta-analyses show exercise has antidepressant effects. They do not show it's a standalone replacement for medication, especially for moderate-to-severe depression. The Schuch meta-analysis itself notes that larger effects were observed in clinical populations receiving exercise as part of a treatment plan. If you're on medication, do not stop or reduce it based on exercise alone. Talk to your doctor.
Misconception: "You need intense exercise to get the mental health benefit"
Reality: Partially true, mostly misleading. Yes, the Noetel 2024 meta-analysis found effects were proportional to intensity. But even light walking showed meaningful antidepressant effects. The difference between doing nothing and doing something is much larger than the difference between moderate and vigorous exercise. If all you can manage today is a 10-minute walk around the block, that counts. Start there.
Misconception: "If exercise hasn't helped my mood, I'm doing it wrong"
Reality: Depression is complex. It has genetic, environmental, social, and biochemical components. Exercise addresses some of these mechanisms, not all of them. If you've been exercising consistently and still struggling, that's valuable information for your healthcare provider, not evidence of personal failure. Some people need medication. Some need therapy. Most benefit from multiple tools working together.

The Consistency Problem (And Why It Matters More Than Modality)
Here's the uncomfortable truth buried in all this research: exercise only works if you do it. Repeatedly. Over time.
That sounds obvious, but it's the critical variable. The Noetel meta-analysis found that strength training and yoga had the highest adherence rates, which is part of why they showed strong antidepressant effects. It's not necessarily that yoga is pharmacologically superior to jogging. It's that people were more likely to keep doing it.
If you've tried to exercise for your mental health and quit after two weeks, you haven't proven exercise doesn't work. You've identified that your approach to consistency didn't work. That's a solvable problem, but it requires a different solution than "try harder."
The research on gamification and exercise adherence is relevant here. Apps and programs that use game mechanics, including progress tracking, rewards, streaks, and adaptive difficulty, consistently produce higher long-term adherence than programs that rely on motivation alone. When it comes to depression specifically, this matters doubly: depression attacks motivation. Building a system that doesn't depend on motivation is the whole point.
What the Research Suggests Going Forward
The evidence is strong and growing stronger. Here's a fair summary of where things stand:
What we know with high confidence:
- Exercise has a large, statistically significant antidepressant effect across hundreds of trials
- The effect is present across exercise types: aerobic, resistance training, yoga, walking
- Higher intensity tends to produce larger effects, but any activity is better than none
- The biological mechanisms (BDNF, serotonin, cortisol reduction, neuroplasticity) are well-documented
- The WHO and major health organizations now include mental health in their physical activity guidelines
What we don't know yet:
- Optimal "dose": exactly how much exercise produces the maximum antidepressant benefit
- Long-term maintenance , most trials run 8-24 weeks; we need more data on multi-year effects
- Individual variation: why some people respond dramatically to exercise while others see modest benefits
- Interaction effects , how exercise combines with medication and therapy in different populations
The honest takeaway: exercise is one of the most powerful, accessible, side-effect-friendly tools available for managing depressive symptoms. It's not the only tool. For many people, it works best when combined with professional support. But dismissing it as "just going for a walk" dramatically undervalues what the research shows.
How FitCraft Helps You Build the Habit
We're not going to claim FitCraft treats depression. It doesn't. It's a fitness app, not a medical device.
What FitCraft does is solve the consistency problem, which, as the research above makes clear, is the problem. The antidepressant effect of exercise requires repeated exposure. A single workout doesn't rewire your brain chemistry. Weeks and months of regular activity do.
FitCraft's free version includes Ty, a 3D AI personal trainer who adapts workouts to your fitness level, equipment, and goals. The programming spans the modalities the research highlights, strength training, yoga, cardio, mobility, and the gamification system (XP, leveling, streaks, collectible rewards) is specifically designed to keep you coming back when motivation dips. Because motivation will dip. That's not a flaw in you. That's biology. Research on fitness apps and mental health shows that the right design approach can lower the psychological barrier to getting started, which is the biggest hurdle for people experiencing depression.
Programs are designed by Domenic Angelino, an Ivy League-trained exercise scientist (MPH, Brown University; NSCA-CSCS) who built the AI coaching engine behind Ty. Every design decision maps to peer-reviewed findings, including the ones in this article.
If you're looking to build a consistent exercise habit and you want something that adapts to you rather than demanding you adapt to it, the free assessment takes two minutes and gives you a personalized starting point.
References
- Schuch FB, Vancampfort D, Richards J, Rosenbaum S, Ward PB, Stubbs B. "Exercise as a treatment for depression: A meta-analysis adjusting for publication bias." Journal of Psychiatric Research 77 (2016): 42-51. doi:10.1016/j.jpsychires.2016.02.023
- Noetel M, Sanders T, Gallardo-Gómez D, et al. "Effect of exercise for depression: systematic review and network meta-analysis of randomised controlled trials." BMJ 384 (2024): e075847. doi:10.1136/bmj-2023-075847
- Singh B, Olds T, Curtis R, et al. "Effectiveness of physical activity interventions for improving depression, anxiety and distress: an overview of systematic reviews." British Journal of Sports Medicine 57.18 (2023): 1203-1209. doi:10.1136/bjsports-2022-106195
- Biddle SJH, Asare M. "Physical activity and mental health in children and adolescents: A review of reviews." British Journal of Sports Medicine 45.11 (2011): 886-895. doi:10.1136/bjsports-2011-090185
- Phillips C. "Brain-Derived Neurotrophic Factor, Depression, and Physical Activity: Making the Neuroplastic Connection." Neural Plasticity 2017 (2017): 7260130. doi:10.1155/2017/7260130
- World Health Organization. "WHO guidelines on physical activity and sedentary behaviour." Geneva: WHO, 2020. who.int
Frequently Asked Questions
Can exercise be as effective as antidepressants for depression?
Research suggests exercise can produce comparable effects. The Schuch et al. (2016) meta-analysis of 25 randomized controlled trials found exercise had a large antidepressant effect (SMD -1.11), and the Noetel et al. (2024) BMJ network meta-analysis of 218 studies confirmed walking, jogging, yoga, and strength training all significantly reduce depressive symptoms. However, exercise should be viewed as a powerful complement to professional treatment, not a replacement, especially for moderate-to-severe depression.
How much exercise do you need to reduce depression symptoms?
The WHO recommends 150-300 minutes of moderate-intensity aerobic activity per week for mental health benefits. Research shows even modest amounts of physical activity reduce depression risk by about 22% compared to inactive individuals. The Noetel et al. (2024) BMJ meta-analysis found effects were proportional to exercise intensity , vigorous exercise produced stronger antidepressant effects than light activity.
What type of exercise is best for depression?
The 2024 BMJ network meta-analysis of 218 studies found walking or jogging (Hedges' g -0.62), yoga (-0.55), and strength training (-0.49) produced the largest reductions in depression. Strength training and yoga had the highest adherence rates. The most effective exercise for depression is the one you'll actually do consistently, which is why personalized, enjoyable programming matters more than any single modality.
How does exercise reduce depression biologically?
Exercise triggers several neurobiological changes that counteract depression. It increases brain-derived neurotrophic factor (BDNF), which promotes neuroplasticity and neurogenesis in the hippocampus. A brain region that shrinks during chronic depression. Exercise also boosts serotonin and norepinephrine availability, reduces cortisol and systemic inflammation, and activates endorphin pathways. These mechanisms overlap with how antidepressant medications work, which helps explain the comparable effect sizes seen in meta-analyses.
Does FitCraft help with mental health and mood?
FitCraft is designed to help you build a consistent exercise habit, which research strongly associates with improved mood and reduced depressive symptoms. The free version includes a 3D AI personal trainer named Ty who adapts workouts to your level, gamification to keep you engaged, and programming that spans yoga, strength training, cardio, and mobility. FitCraft isn't a mental health treatment, but the consistent physical activity it helps you maintain is one of the most evidence-backed tools for emotional well-being.